| UW MSK Resident Projects |
|
|
|
|
ACL ReconstructionPrint-friendly version of this page
by Dawn Hastreiter, M.D., Ph.D. In the beginning .... In order to have an ACL reconstruction, you first need to have an ACL tear. Symptoms of an ACL tear include: pivot shift episodes, pain, and feeling a 'pop.' On physical exam, the physician usually finds an effusion, a positive anterior drawer sign, a positive Lachman's test, and/or a positive pivot shift test. MR has a greater than 90% sensitivity and specificity for detecting a ruptured ACL (3). Tears are best demonstrated on T2 MRI sequences. The characteristics of ACL disruption are as follows:
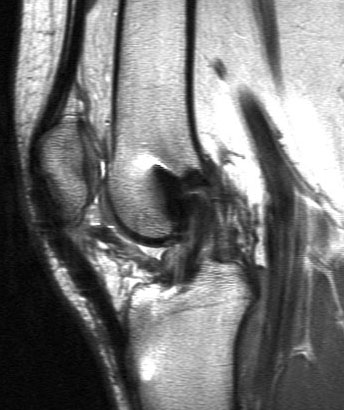
Joint space findings can also provide clues as to an ACL tear. These include effusion, posterior cruciate ligament (PCL) angulation, anterior subluxation, bone bruise, Segond fracture, uncovered lateral meniscus, deep femoral notch, MCL tear, and meniscal tear (2-3). Figure 1 demonstrates an ACL tear seen at MRI.
Figure 1. Sagittal MRI of the knee showing a complete ACL tear.
Types of Reconstruction Today, reconstruction is usually done without an open knee surgery. It is performed with arthroscopic assistance and running a graft through reamed tunnels in the tibia and femur. The graft is generally anchored at both ends. Graft materials are more often harvested from the patient, but cadaver grafts are still used in select patients. Prior to graft placement, the existing torn ACL must be arthroscopically debrided out of the knee thoroughly.
One common method of reconstruction uses a central third patellar-tendon autograft. The middle one third of the ipsilateral patellar tendon is harvested with bone plugs from the patella and tibial tuberosity. The graft is inserted through femoral and tibial tunnels. It is often secured by two metal or absorbable interference screws. An animation of how this procedure is performed can be found here. Follow the links for examples of how this reconstruction appears in AP and lateral plain x-rays (15).
Another method of reconstruction, favored at the University of Washington currently, uses a double loop graft of semitendinous and gracilis tendons. In this procedure, portions of the hamstring tendons are dissected from their muscular insertion. Their bony insertion remains intact. The graft is then pulled through the tunnels and looped back over an Endobutton in the femur, thus becoming a double loop. The lower portion is secured with a screw in the tibia. The EndoButton is a metal flat washer (what we see on x-ray) attached to a loop of polyester tape through which the graft is run. An animation of how this procedure is performed can be found here, except that an EndoButton is used instead of a screw to secure the loop in the femur. Figure 2 shows how this reconstruction appears on plain x-rays.
Figure 2. AP and lateral views of an ACL reconstruction performed using a hamstring autograft.
Causes of Failure and Complications of ACL Reconstruction
Causes of graft failure can be divided into three categories: technical, biologic, and external (5). Technical causes include nonanatomic tunnel placement, hardware failure, bone plug fracture, inadequate notchplasty, improper tensioning, graft fixation, and insufficient graft material. Plain x-rays can be used to evaluate fracture of the bony portions of the grafts, metallic screw integrity and position, union of the bony portions of the graft, tunnel placement, and size of screw tunnels. MR can also be used to evaluate tunnel positioning, graft integrity, the other soft tissues of the knee. The femoral tunnel should be at the intersection of Blumensaat's line (intercondylar roof line) and a line extended from the posterior femoral cortex. Tibial tunnel placement should be posterior and parallel to the tibial intersection of Blumensaat's line. One of the more common problems with the tunnels is placement that is too anterior (15). Tunnels may enlarge over time but this does not seem to affect outcome (1). Screw placement does not necessarily correlate with the tunnel lines. Osseous incorporation of the patellar tendon grafts occurs by one year in most cases (1, 11). On MR, an intact unimpinged graft should have homogenous low signal. It should be posterior to and not in contact with the intercondylar roof (14). Grafts impinging on the roof or sidewall will have irregular increased signal (6). Due to metal artifact on T2 images, T1 may be more useful for assessing technical failure (2).
Biologic causes for failure include: failed ligamentization (for those grafts which were not originally ligaments), infection, arthrofibrosis, and infrapatellar contracture syndrome. Arthrofibrosis is a loss of extension of more than 10 degrees or flexion of greater than or equal to 15 degrees. It could be caused by a cyclops lesion. This is a fibrous nodule anterolateral to the tibial tunnel that impinges on the intercondylar notch when the knee is extended (Figure 3). It causes an abrupt endpoint of extension with a popping sensation. The cyclops lesion could result from drilling debris, ACL stump remnants, broken graft fibers, or repeated impingment of the graft on the notch (4). Adequate notchplasty (anterolateral debidement of the tibial tunnel) is required to reduce the rate of cyclops formation, which can occur in as many as 5-10% of patients (12). A cyclops lesion is seen on MR as a low-signal intensity nodule outlined by fluid.
Figure 3. Sagittal MR of the knee demonstrating a cyclops lesion.
External causes for failure include: traumatic rupture, secondary instability of the knee, and improper rehabilitation (5). Graft rupture, similar to native ACL rupture, is best demonstrated on MRI as has been described (Figure 4). Caution is advised when using secondary signs of ACL rupture since some of these are normal in a post-operative state, such as an effusion (1).
Figure 4. Sagittal MR of knee demonstrating failed graft. The fibers are disrupted and there is high signal intensity in the graft substance.
Osteoarthritis (OA) is a common complication of ACL reconstruction and can be imaged by plain x-rays. Changes usually can be seen by 7 years post-operative (8-9, 12). A recent study showed that patellofemoral OA is more common than tibiofemoral OA (47% vs. 14-18%) an average of 7 years post-operative (7). In this study, the patellofemoral OA corresponded in severity to degree of shortening of the patellar tendon. The OA is more advanced in those patients for which the ACL injury was chronic (> 12 weeks) prior to surgery and when meniscectomy was required (8-9, 12).
Subsequent surgery is not an infrequent complication of ACL reconstruction. Meniscectomy can later be needed in a small percentage of patients (9, 12). Screw removal can also be required in as many as 10% of patients (9). This might be necessary due to patient pain or that the screws may back out as the bone heals and affect cosmesis. Debridement procedures could be required for adhesions, arthrofibrosis, or cyclops lesions.
Other knee injuries can complicate an ACL repair. These include associated tendon injuries, meniscal injuries requiring surgery, patellar tendonitis, patellar tendon rupture, and patellar fracture. The latter three would be seen with the patellar tendon grafts. Patellar fracture can be detected with plain x-rays. Derangement of the soft tissues structures can be seen on MRI.
Outcome
Short term success of ACL reconstruction is generally very good. Data is limited on long term success of many of the procedures employed today. An additional traumatic injury seems to be the most common cause of reoperation now that many of the technical problems of the surgery have been perfected. For patellar tendon grafts, approximately 4-10% have traumatic rupture in 5-7 years (9, 12).
In the case of patellar tendon grafts, the central third of the patellar tendon reconstitutes after 12-18 months, as has been demonstrated by MRI (12). The patellar tendon can remain increased in thickness. Absorbable interference screws are generally resorbed by 1 year (1) and can be seen on MRI.
References
1. Bach, FD, et al. Anterior Cruciate Ligament Reconstruction with Bioabsorabable Polyglycolic Acid Interference Screws: MR Imaging Follow-up. Radiology. 2002; 225: 541-550. 2. Berquist TH. Knee. In MRI of the musculoskeletal system. Philadelphia: Lippincott Williams & Wilkins, 2001. 3. Chan WP, Peterfy C, Fritz RC, Genant HK. MR Diagnosis of Complete Tears of the Anterior Cruciate Ligament of the Knee: Importance of Anterior Subluxation of the Knee. AJR. 1994; 162: 355-360. 4. Delincé P, Karallis P, Descamps P-Y, Fabeck L, Hardy D. Different Aspects of the Cyclops Lesion Following Anterior Cruciate Ligament Reconstruction: A Multifactorial Etiopathogensis. Arthroscopy. 1998; 14: 869-876. 5. Getelman MH, Feidman MJ. Revision Anterior Cruciate Ligament Reconstruction Surgery. J Am Acad Orthop Surg. 1999; 7: 189-198. 6. Howell SM, Berns GS, Farley TE. Unimpinged and Impinged Anterior Cruciate Ligament Grafts: MR Signal Intensity Measurements. Radiology. 1991; 179: 639-643. 7. Järvela T, Paakkala T, Kannus P, Järvinen M. The Incidence of Patellofemoral Osteoarthritis and Associated Findings 7 Years After Anterior Cruciate Ligament Reconstruction with a Bone-Patellar Tendon-Bone Autograft. Am J Sports Med. 2001; 29: 18-24. 8. Jomha NM, Borton DC, Clingeleffer AJ, Pinczewski LA. Long Term Osteoarthritic Changes in Anterior Cruciate Ligament Reconstructed Knees. Clin Orthop Related Res. 1999; 358: 188-193. 9. Jomha N., Pinczewski L, Clingeleffer A, Otto D. Arthroscopic reconstruction of the anterior cruciate ligament with patellar-tendon autograft and interference screw fixation: The results at seven years. JBJS (Br). 1999; 81-B: 775-779. 10. Magee TH, Hinson GW. MRI of meniscal bucket-handle tears. Skeletal Radiol. 1998; 27: 495-499. 11. Manaster B, Remley K, Newman AP, Mann FA. Knee Ligament Reconstruction: Plain Film Analysis. AJR. 1988; 150: 337-342. 12. Patel JV, Church JS, Hall AJ. Central Third Bone-Patellar Tendon-Bone Anterior Cruciate Ligament Reconstruction: A 5-Year Follow-up. Arthroscopy. 2000; 16: 67-70. 13. Recht, MP, and J Kramer. MR Imaging of the Postoperative Knee: A Pictoral Essay. RadioGraphics. 2002; 22: 765-774. 14. Recht MP, Piranino DW, Applegate G, et al. Complications After Anterior Cruciate Ligament Reconstruction: Radiographic and MR Findings. AJR. 1996; 167: 705-710. 15. Wheeless' Textbook of Orthopaedics. Anterior Cruciate Ligament.
|




{kind=link}
{kind=link}
{kind=link}
|