| UW MSK Resident Projects |
|
|
|
|
Ankylosing SpondylitisPrint-friendly version of this pagePosted by cjhurt@u.washington.edu, 10/19/04 at 6:31:40 AM.
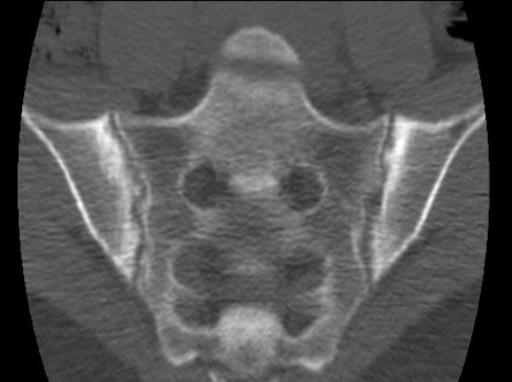
When deciding to write one of these stories, the last thing I wanted to do was to write a long story. I've read a lot of long stories, but very little of long stories seem to stick around. I figured by choosing a zebra, that would allow a quick chat, rather than a story, as not much literature would be around from which to draw, say, on POEMS syndrome. Sigh... Instead, I'll try to write something pithy about a common entity. I'll try to keep this simple since we'd all prefer it that way. Moreover I figure what we're all interested in is the radiologic stuff, so that's what I'll mainly talk about. Ankylosing spondylitis (AS) represents a chronic inflammatory disease, primarily affecting the axial skeleton and secondarily affecting the appendicular skeleton. It typically presents in men, 15-35 years old. Remember it as the least erosive and most ossifying arthropathy. Joint ankylosis is the hallmark, as the name less than subtlely suggests. Some details on different pieces of anatomy: SI joints are radiographically invovled first, bilaterally and symmetrically. Joint edges have a serrated "postage stamp" appearance due to tiny erosions, which start on the iliac side, due to the thinner cartilage, then progress to the sacral side. Here's a CT example that gives you an idea of the fine nature of the erosions:
Erosions are much less than seen with other spondyloarthropathies. Further down the line you might see something like this:
The synovial portion of the SI joint, i.e. the anteroinferior 1/2 to 2/3 of the joint, ankyloses first, follwed by the ligamentous portion. Ankylosis of the posterosuperior ligamentous portion is considered to look like a "star." The first CT above gave you an idea of the initial involvement of the anteroinferior SI joint portion, while the next CT shows the more diffuse involvement at a later stage. Obviously the end result is ankylosis, which we see starting here on CT: and here on a plain radiograph:
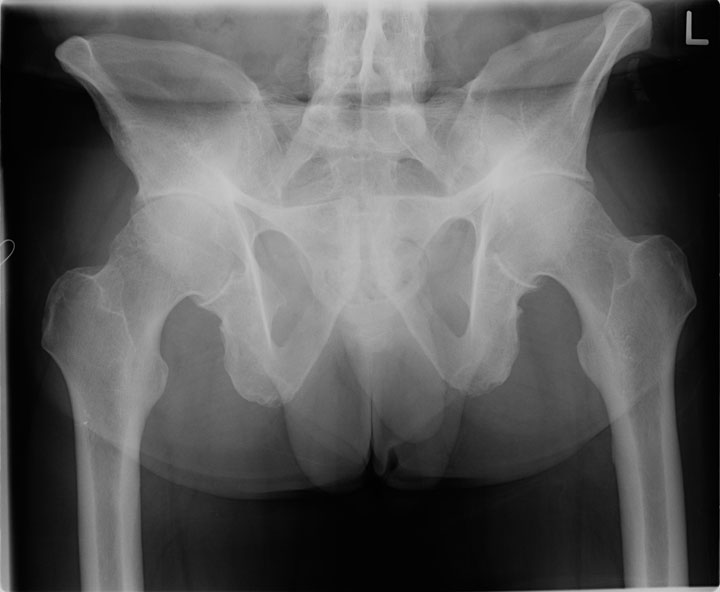
Other findings you might see in the pelvis, if you're not overwhelmed by those SI joints and a glimpse of the spine, are ossification of ligamentous attachments in the iliac crests and ischial tuberosities, classically giving a purported "whiskered" look. That sounds cute doesn't it. Looks just kind of fuzzy to me. The symphysis pubis can show tiny "serrated" erosions like the SI joints, before it ankyloses. Purportedly, ~25% of ankylosing sponylitis eventually has symphysis pubis involvement. Probably since SI joints are the first radiographic evidence of AS and the pelvis is being imaged for that, lumbosacral AS involvement is typically seen first, as we see on the above pelvis radiograph, although apparently the thoracolumbar junction can be the first site of invovlement in the spine for AS. Involvement progresses cranially to involve the entire spine. At first, there is slight erosion of the vertebral body corners with secondary sclerosis, giving a classic squared vertebral body with "ivory" corners. We see those pearly whites nicely here: The ivory corners disappear, not unlike true elephant ivory has, leaving simply square vertebral bodies. There is an explanation for these ivory corners, even if I can't explain where all the elephants' ivory went. The outer portion of the annulus fibrosus, i.e. Sharpey's fibers, ossify first. Apparently this may not always be seen radiographically, but decreased ROM will suggest this to an astute radiologist. The ossification progresses deeper to involve the longitudinal ligaments, resulting in the classic syndesmophyte seen with AS, linking adjacent vertebral bodies. Here we see a nice AP and lateral example of 'dem syndesmophytes:
Disc spaces tend to remain normal at first, with no loss of height,
but they may eventually calcify. Apophyseal joints in the spine can be
involved, if they choose to, with resultant erosions followed by
ankylosis. All spinal ligaments can eventually ossify giving the
classic "bamboo" spine. Now I just made my pet panda hungry.
Once you get a bamboo spine, a classic sign is that of the "tram track," namely the syndesmophytes and ossified ligaments between spinout processes look like "tram tracks." We get a hint of that here in the pelvis, which we saw above, in case you're paying attention:
as well as here:
Although this last one seems more like a Monorail. For further details on tram tracks, talk to MSK Fellow Durkee, as he does a thorough job at explaining trams. One point to remember, as forgetting it could give grave results, is that odontoid erosions can be seen with AS. Atlantoaxial subluxation can be seen as well. So, don't jump to conclusions and label someone with "arthritis" and such cervical findings with RA, when in fact they may have AS. The bamboo spine, though, would probably give away the diagnosis. Although the odontoid is still present and accounted for, here's a nice example of an AS C-spine:
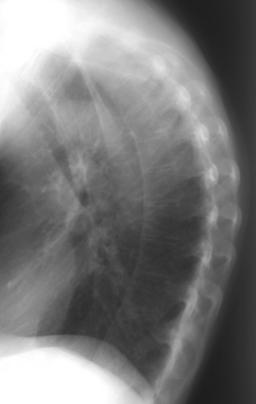
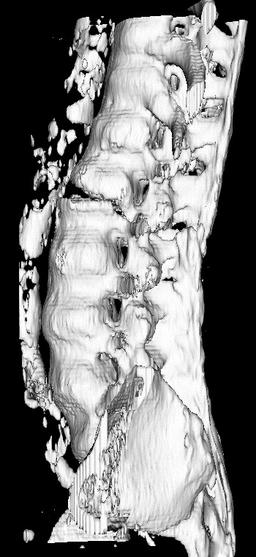
A couple of things to be aware with AS. As with DISH, intubating someone with an ankylosed C-spine can result in horrendous fracture with paralyzing results. Similarly, fracture in the thoracolumbar region can result in pseudoarthrosis. This can also result from an area that failed to ossify. At this area one can see DDD, erosion, and bony sclerosis. These findings can resemble severe DDD, discitis/osteomyelitis, or "neuropathic" spinal disease. Now that you are aware of the possibility of pseudoarthrosis, you can consider that as a possible diagnosis too. Here's a neat example of pseudoarthrosis:
with a CT 3D recon for grins too:
Moving beyond the axial skeleton, the hip is the most common appendicular joint involved. Two kinds of patterns can be seen when the hip is involved, i.e. nondestructive and destructive. Kind of reminds me of relationships. The former is fortunately more common, as hard as that is to believe sometimes. In AS the hips are involved bilaterally and symmetrically, with, surprise surprise, ankylosis being the characteristic feature. There can be no joint space loss, or uniform joint space loss with axial migration of the femoral head. Here's a fine example of the uniform joint space loss and axial migration:
Tiny erosions can be seen, but overall the femoral head contour is preserved. Pre-ankylosis there will be a osteophyte collar with normal mineralization, while post-ankylosis the phytes go byebye and the bones become osteopenic. The destructive hip is unilateral and insidious, resulting in marked destruction of the femoral head prior to ultimate ankylosis. The shoulder is the next most frequent appendicular joint involved. Again we see destructive and nondestructive patterns. With the latter there is a normal humeral head ankylosed to the glenoid with much ossification of the coracoclavicular ligament. With the destructive type there is a "hatchet" erosion of the humeral head. Not that I know what a hatchet blow looks like, but I think sometimes I could benefit from having such a weapon. Here's a neat example of hatcheting:
With the hatchet shoulder, ankylosis will eventually occur after much destruction has been wreaked. The knee is involved in ~30% of longstanding cases, not because they're standing, but, well you know what I mean. The AC, sternoclavicular, and sternomanubrial joints can all be involved. Purportedly only ~10% of longterm AS shows elbow, hand, and feet involvement. In all of these less involved joints, erosions, if present at all, are slight, with minimal bone sclerosis, but as you guessed, intra-articular ankylosis is the characteristic. Progression of an ankylosing joint tends to be rapid. Da capo... No, just kidding, unless you perseverate. I really meant to say these are the take home points:
Brower's summary in her classic book: Arthritis in Black and White (2nd ed. Philadelphia, W.B. Saunders, 1997.) is also a great start for getting the skinny on AS. Additional classic AS reads:
|









|