| UW MSK Resident Projects |
|
|
|
|
Enchondromas and Related DisordersPrint-friendly version of this pagePosted by jkanne@u.washington.edu, 5/17/04 at 8:52:19 AM.
What are they?
Enchondromas are benign cartilaginous neoplasms that originate in the medullary canal of tubular bones, believed to result from growth of residual benign cartilage rests displaced from the physis. They are often incidental findings, occurring in just under 2% of the population based on autopsy series.
Where do they occur?
Approximately half of all enchondromas occur in the tubular bones of the hands and feet, with others are found in the metaphyses of other long bones. They rarely occur in the pelvis, shoulder girdle, and axial skeleton.
What do they look like?
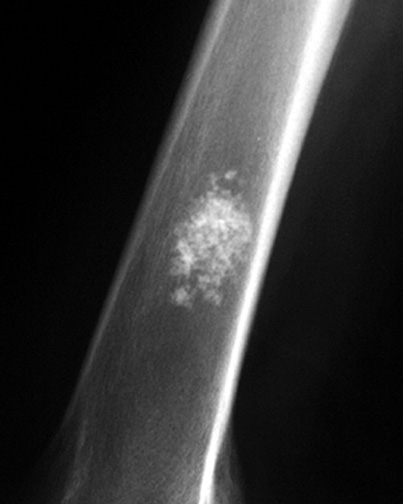
Radiographically, enchondromas appear as geographic, mildly expansile, lytic lesions, which may lead to mild cortical thinning. The zone of transition is narrow, although it can be lobular. A cartilaginous matrix (rings and arcs) is often present, less often in lesions occurring in the hands and feet. There is no cortical break through or host response in the absence of fracture. Enchondromas are usually monostotic, although multiple lesions can occur in the feet and hands. On MR, they have typical signal characteristics of chondroid lesions with low signal on T1 and very high signal on T2 (due to high water and mucopolysaccharide content).
Fig 1. Enchondroma in the distal femur. Note the lesion is geographic with response from surrounding bone. Cartilagenous matrix is present.
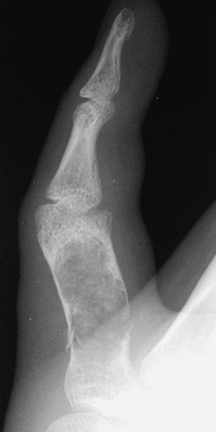
Fig 2. Enchondroma in the hand. A pathological fracture has developed.
Differential diagnosis:
Enchondromas are usually easy to characterize. However, other diagnostic considerations include: Hands and feet: epidermoid inclusion cyst, giant cell tumor, aneurismal bone cyst, simple bone cyst, and fibrous dysplasia. Other sites: infarction, chondromyxoid fibroma (rare, generally lacks matrix, and favors the proximal tibia). The more difficult diagnostic dilemma is distinguishing enchondroma from low-grade chondrosarcoma. The latter are usually larger, occur in less typical places, generally occur more proximal, and may have deeper and more pronounced endosteal scalloping. More importantly, local pain related to the lesion is always concerning for malignancy.
Complications:
Pathologic fracture and malignant transformation (the latter is rare in enchondromas of the feet and hands).
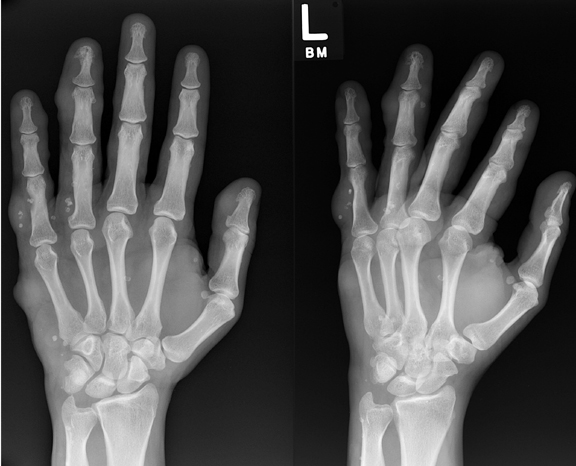
Fig 3. Transformation of enchondroma into a chondrosarcoma. Note the periosteal reaction indicating a host response.
Related disorders:
Ollier's disease is a rare developmental disorder characterized by enchondroma formation in the metaphyses and diaphyses of multiple long bones, typically unilateral and involving one extremity. Ollier's disease is not hereditary or familial. It usually presents early with deformed epiphyses. The enchondromas of Ollier's disease may have different radiographic manifestations than those of classic enchondroma with striated lucency and densities and most have some chondroid matrix. Risk for malignant transformation is believed to be around 10-25%.
Maffucci's syndrome is defined as multiple enchondromatosis with soft tissue and visceral hemangiomas. Patients with Maffucci's syndrome are believed to be at far greater risk for malignant transformation than those with Ollier's disease.
Fig 5. Maffucci's syndrome. Soft tissue masses with phleboliths are consistent with hemangiomas. Note remodeling of underlying bone.
References:
|




|