| UW MSK Resident Projects |
|
|
|
|
HyperparathyroidismPrint-friendly version of this pagePosted by adam_myhre@yahoo.com, 1/20/04 at 8:49:38 AM.
What is it? Parathyroid hormone is the main hormone that maintains a balance of calcium and phosphate in our bodies. When
released, parathyroid hormone increases the release of calcium from the
bone, reabsorption from the kidney, and secondarily stimulates
absorption of calcium from the intestines. It also stimulates secretion of phosphate in the kidney. Hyperparathyroidism is the abnormal secretion of parathyroid hormone. Clinical findings: The classic medical
school clinical findings are "Stones, Bones, abdominal moans, and
psychiatric overtones," referring to renal calculi, bone pain, peptic
ulcers, pancreatitis, and CNS symptoms (confusion lethargy, weakness). Depending on the etiology, the serum calcium may be elevated and phosphate may be decreased. Etiology: Primary Hyperparathyroidism Excessive parathyroid hormone due to a parathyroid gland abnormality 80% parathyroid adenoma 12% parathyroid hyperplasia (rarely from Multiple endocrine neoplasia) 1-3% parathyroid carcinoma Secondary Hyperparathyroidism Excessive parathyroid hormone due to an abnormality elsewhere in the body. Most often this is
from chronic renal failure where elevated phosphate and +/- decreased
calcium lead to chronic stimulation of the parathyroid gland. Tertiary Hyperparathyroidism Excessive parathyroid hormone due to autonomous secretion of parathyroid hormone. Often this is from prolonged secondary hyperparathyroidism from renal failure. Then,
when the patient receives a renal transplant, cause of the secondary
hyperparathyroidism is taken away, but the parathyroid glands continue
to over secrete parathyroid hormone. Radiology of Hyperparathyroidism Osteopenia and bone demineralization are present in all forms of hyperparathyroidism Subperiosteal resorption
is virtually pathognomonic for hyperparathyroidism and is typically
seen at the radial aspect of the middle phalanx of the index and middle
fingers Figure 1: Subperiosteal resorption as well as acroosteolysis, the next sign of hyperparathyroidism Figure 2: Subperiosteal resorption in a child Figure
3: Compare the finger on a patient with
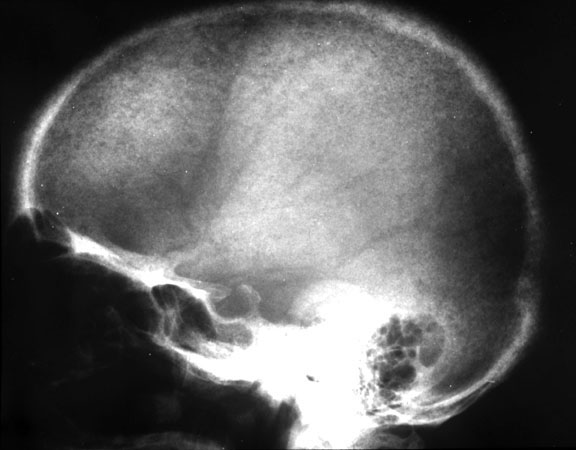
hyperparathyroidism, to his normal appearing finger after treatment Phalangeal tuff resorption/acroosteolysis Figure 4: Acroosteolysis (also subperiosteal resorption) Acroosteolysis differential diagnosis Mnemonic from The Primer: (Presented because I can never remember it) PINCH FO Psoriasis Injury (thermal/frostbite) Neuropathy (congenital insensitivity to pain, diabetes, leprosy, myelomeningocele) Collagen vascular disease (Scleroderma, Raynaud's) Hyperparathyroidism Familial (Hadju-Cheney) Other (Polyvinyl chloride exposure, snake/scorpion venom) Subchondral resorption Sacroiliac joints Distal clavicle Pubic symphysis Salt and pepper skull Figure 5: Salt and pepper skull Figure 6: Normal skull in the same patient following treatment of hyperparathyroidism Brown Tumor Brown tumors are more
common in patients with primary hyperparathyroidism, however, due to
the increased prevalence of secondary hyperparathyroidism, there are
more brown tumors from secondary hyperparathyroidism than form primary
hyperparathyroidism. It is difficult to
differentiate a Brown Tumor from a giant cell tumor or fibrous
dysplasia; however, other signs of hyperparathyroidism should be
present. Figure 7: Brown tumor in the phalanx (also subperiosteal resorption, tuft resorption, and osteopenia) Figure 8: Brown tumor in the inferior obturator ramus Soft tissue calcification Primary > Secondary Chondrocalcinosis Secondary > Primary Knee Triangular fibrocartilage Symphysis Pubis
Osteosclerosis Secondary > Primary
Periostitis Secondary > Primary
Tendon and ligament laxity May lead to rupture
Renal osteodystrophy General term for the radiology changes associated with renal failure
Secondary hyperparathyroidism (as describe above)
Also includes: Osteomalacia (Normal osteoid, abnormal mineralization) 1. Demineralized coarsened bones 2. Looser's zones Axillary margin of the scapula Inner femoral neck Ribs Pubic and ischial rami
Figure 9: Looser's zones in the inferior femoral neck
Osteosclerosis Rugger Jersey spine
Figure 10: Rugger Jersey spine
Soft tissue calcification Vascular calcification
Images:
Drs. Escobedo's, Hunter's, and Richardson's teaching files.
References:
Cooper KL. Radiology of metabolic bone disease. Endocrinology Metabolism Clinics of North America. 1989; 18(4): 955-76.
Manaster BJ, et al. Musculoskeletal Imaging: the Requisites. Second Edition. Mosby, 2002.
Weissleder R, et al. Primer of Diagnostic Imaging. Second Edition. Mosby, 1997.
|











|