| UW MSK Resident Projects |
|
|
|
|
Spectrum of Medial Collateral Ligament InjuryPrint-friendly version of this pagePosted by jamillan@u.washington.edu, 3/29/04 at 10:53:48 AM.
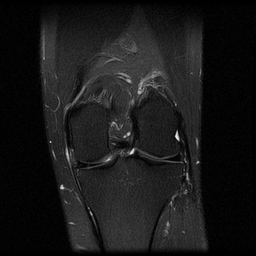
MEDIAL COLLATERAL LIGAMENT(ANATOMY): The medial collateral ligament is typically divided into the superficial and deep bands. The superficial portion of the ligament typically arises from the medial femoral condyle and passes distally to insert approx. 5cm below the joint line and posterior to the pes anserinus on the medial aspect of the proximal tibia. Superficial fibers are separated from the deep fibers by a bursa. The deep ligament is firmly attached to the capsule and the midportion of the medial meniscus and attaches to the femur and tibia adjacent to the joint. The medial collateral ligament is a stabilzer that resists external rotation and anterior forces and is more often injured than its lateral counterpart. Click here for anatomy link for Medial Collateral Ligament anatomy from Wheeless' Textbook of Orthopaedics. HOW DOES IT OCCUR? This injury usually occurs when a blow to the outer side of the knee causes stretching or tearing of the medial collateral ligament. It can also be caused by twisting the knee. Specifically, the ligament is injured due to a valgus stress with the knee in flexion. GRADING INJURY: TYPES OF MEDIAL COLLATERAL LIGAMENT INJURY(GRADE I-III): Three appearances of the MCL with T2 Weighted Images. I. A sprain, shows high T2 signal in the soft tissues medial to the MCL.
II. A severe sprain or partial tear, shows high signal in the soft tissues medial to the MCL, but also has high signal or partial disruption of the MCL itself. As well, there can be thinning of the MCl itself.
III. A complete tear, shows complete disruption of the MCL.
ASSOCIATED INJURIES: Associated injuries of the capsule specifically meniscocapsular separation, and can be diagnosed by noting fluid between the MCL and the medial meniscus. Additionally, injuries of the anterior cruciate ligament are also commonly seen with these injuries. Commonly seen injury is so named the UNHAPPY TRIAD: 1. ANTERIOR CRUCIATE LIGAMENT TEAR 2. MEDIAL COLLATERAL LIGAMENT INJURY 3. MEDIAL MENISCUS TEAR WHAT IS THE TREATMENT FOR A MEDIAL COLLATERAL LIGAMENT INJURY? When a grade II MCL sprain occurs, use of a hinged knee brace
is common in early treatment. Athletes with a grade II injury can
return to activity once they are not having pain over the MCL. When a
grade III injury occurs, patients usually wear a hinged knee brace and
protect weight-bearing with a gradual return to normal activities.
Patients with more severe injuries usually require physical therapy and
will not return to their full level of activity for 3 to 4 months. References:
|


|