| UW MSK Resident Projects |
|
|
|
|
Osteochondral DefectPrint-friendly version of this pagePosted by jimmwong@u.washington.edu, 11/5/03 at 9:16:35 PM.
Pathophysiology:
Osteochondral defect (OCD) (old name = osteochondritis dissecans) may result directly from trauma or secondarily from loss of blood supply to an area of subchondral bone, resulting in avascular necrosis. The overlying cartilage, which is nourished by synovial fluid, remains intact to variable degrees. As the necrotic bone is resorbed, the overlying cartilage looses its support. Without its cartilage cover, the bony fragment may become dislodged into the joint. Although trauma is thought to be the inciting event, a discernable cause is identified in only a minority of cases (21-40%). Repetitive microtrauma is likely the cause of the majority of cases.
Epidemiology:
Overall incidence of osteochondral defect in the general population is estimated to be 15 to 30 per 100,000 people. Males are involved 3 times more often than females. Average age at presentation is 10-20 years, but OCD may occur at any age. Involvement is bilateral in 30-40% of cases.
Distribution:
The first three are in decreasing order of frequency.
Knee (75% of cases): Lateral aspect of the medial femoral condyle (75%) Weight-bearing surface of medial femoral condyle (10%) Weight-bearing surface of the lateral femoral condyle (10%) Anterior intercondylar groove or patella (5%)
Elbow: Anterolateral aspect of the capitellum is the most common site in the elbow.
Ankle: 4 to 14 times more common in the talus (56% posteromedial, anteromedial 44%) than the tibial plafond.
Rare sites: Tarsal navicular, femoral capital epiphysis, shoulder (humeral head and glenoid), scaphoid.
Radiographic findings:
Conventional radiographs: May be normal. When visible, seen as lucencies in the articular epiphysis (which may have a well-demarcated rim of sclerosis) or loss of sharp cortical line of the articular surface. Plain films cannot adequately evaluate assess articular cartilage and stability.
Computed tomography: Island of subchondral bone demarcated by a rarefied zone.
Magnetic resonance imaging: All abnormalities on plain film or CT should be evaluated for stability by MRI. MRI is the most accurate method for staging lesions (short of arthroscopy).
MRI classification of OCD:
I. Marrow edema (stable). II. Articular cartilage is breached. Low-signal rim surrounding fragment indicates fibrous attachment(stable). III. Pockets of fluid around undetached and undisplaced osteochondral fragment (unstable). IV. Displaced osteochondral fragment (unstable).
Arthrography (CT or MR): Arthrography provides additional information about size of lesion and can assess stability of lesion and integrity of overlying cartilage.
Nuclear medicine: Nonspecific mild to marked increased uptake in involved bone.
Management:
Conservative treatment (low-intensity physical rehabilitation) is recommended for stable (stages I and II) lesions. If symptoms worsen or fail to improve or crepitus (suggesting detachment) develops, then arthroscopy is recommended to evaluate stability of the lesion. Depending on findings at arthroscopy, a loose body may be removed, a fragment may be excised, cartilage may be debrided, or lesion may be drilled to promote revascularization.
Case:
AP view of the elbow demonstrates a well-defined lucency in the capitellum.
Coronal T1-weighted image of the elbow demonstrates a low-signal lesion corresponding to finding on plain radiograph.
Coronal fat-suppressed T2-weighted image demonstrates no fluid surrounding the fragment, suggesting stability.
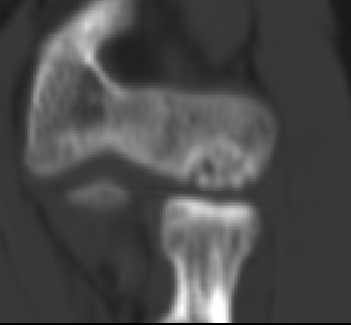
Coronal reformation of CT performed prior to intra-articular injection of contrast demonstrates a well-defined area of heterogeneity abutting the articular surface.
Coronal reformation of CT performed with intra-articular contrast demonstrates no contrast surrounding fragment, suggesting stability |




|