| UW MSK Resident Projects |
|
|
|
|
Paget's Disease (Osteitis Deformans)Print-friendly version of this pagePosted by shawniep@u.washington.edu, 7/1/04 at 9:07:42 AM.
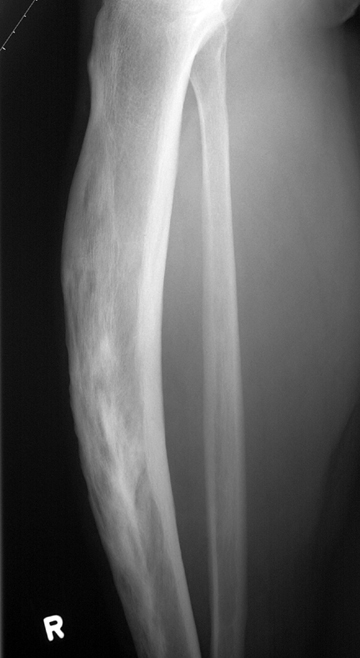
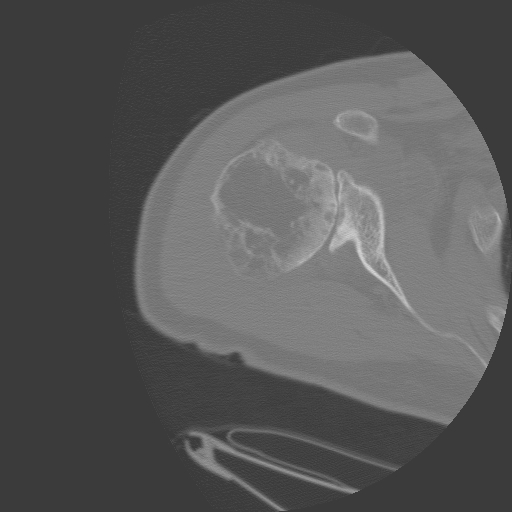
Paget's Disease (Osteitis Deformans) What is it? Paget's disease is a chronic progressive focal disease of bone, characterized by excessive resorption followed by excessive formation of bone, with abnormal bone remodeling. This process results in mosaic pattern of lamellar bone, with extensive local vascularity and increased fibrous tissue in the bone marrow. Involvement is usually polyostotic and asymmetric, and prefers the pelvis, spine, skull, femur, and tibia. Three phases: 1) "hot" or "active" phase (osteolytic dominant, with fibrous replacement of marrow and vascular hypertrophy); 2) "mixed" phase (disorganized lamellar bone deposition plus osteolysis; rapid bone turnover); 3) "cold" phase (osteoblastic dominant; pagetoid woven bone replaced by islands of lamellar bone, but haversian systems and remodeling along lines of stress do not occur). Who gets it and why? Hard to accurately say who is affected because many affected individuals are asymptomatic, but autopsy studies have shown approximately 3% of adults over 40 have the disease. Unusual under age 40. Unknown etiology, probably viral. Clinical Findings: Often asymptomatic, but can have a painful, warm extremity, bowing of long bones, high output CHF, enlarged hat size, sequelae from spinal cord/nerve compression, and elevated serum alkaline phosphatase and urine hydroxyproline.Radiographic Features: Plain films: Lysis typically begins at an epiphysis and slowly advances at rate of a few mm per year to involve entire bone. Classically described as a "candle flame" or "blade of grass" lesion, with lucent osteolytic advancing edge, and sharp transition between normal and involved bone. Pagetoid (woven) bone forms behind advancing osteolysis, with coarsened trabeculae and overall decreased cortical density. Not uncommon to see insufficiency fractures and deformities because of lack of bone remodeling.
Spine: Classic lesion is the "picture frame" appearance of the vertebral body, with initial widening of the peripheral cortex. This progesses to a dense sclerotic body with continued endosteal progression, and eventually even the posterior elements are involved. Skull: Commonly involves cranial vault. Well demarcated geographic appearance ("osteoporosis circumscripta") in lytic phase (particularly frontal bones), followed by focal radiodensities with pagetoid bone formation, and finally a thickened radiodense "cotton wool" appearance in the quiescent phase. Basilar invagination can be seen due to insufficiency of the pagetoid bone; subsequent narrowing of neural foramina and foramen magnum can occur. Pelvis: Thickening of the iliopubic and ilioischial lines early in the disease, with subsequent trabecular thickening and acetabular protrusio.
Long bones: Cortical thickening and bone enlargement. Bowing of tibia and femur.
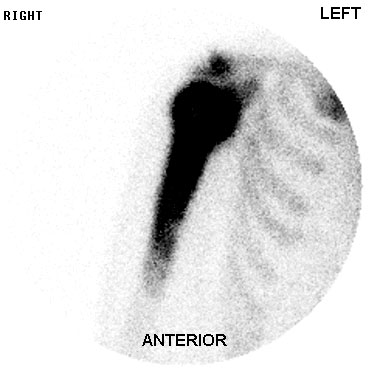
-Helpful in determining extent of disease. -Extremely hot in lytic phese; can be cold if inactive (uncommon). -Increased radiotracer uptake usually abuts on joint and extends distally.
Complications: Fractures: Secondary to insufficiency, often incomplete. Neoplasm: Sarcomatous degeneration is rare (<1%), but more likely with extensive disease.
Differential Diagnosis: Main consideration is metastatic disease, which much more commonly involves ribs than Paget's. Treatment: Goal is to arrest the osteolytic process. 1) Calcitonin (inhibits bone resorption) 2) Disphosphonates (inhibit demineralization) 3) Mithromicin (cytotoxic antibiotic) References: 1. Metabolic Bone Disease and Clinically Related Disorders, Third Edition. Avioli, L and Krane, S, Eds. c 1998, Academic Press, San Diego, CA. pp 545-596. 2. Musculoskeletal Imaging- The Core Curriculum Serie . Chew, F. c 2003, Lippincott, Williams & Wilkins, Philadelphia, PA. pp 478-484. 3. Primer of Diagnostic Imaging, Second Edition. Weissleder, R, Rieumont, M, and Wittenberg, J. c 1997, Mosby, St. Louis, MO. pp 428-9.
Several photographs are courtesy of Dr. Hunter and Dr. Richardson's web sites. |





|