| Home
About
|
Peroneal Tendon Injury
Print-friendly version of this page
Posted by mpsmith@u.washington.edu, 9/19/04 at 10:20:40 PM.
Peroneus Brevis and Peroneus Longus Tendon Injuries
ANATOMY
- The P. longus muscle originates on the proximal and mid lateral fibula and fans along the the plantar surface of the foot to insert on the plantar aspect of the base of the 1st metatarsal and the medial cuneiform
- The P. brevis muscle originates on the mid and distal lateral fibula and inserts on the base of the 5th metatarsal
 
Fig. 1 Peroneus Longus (left) and Brevis (right) Muscles
- The brevis and longus tendons are located on the posterolateral aspect of the ankle, passing posterior and inferior to the lateral malleolus
- The tendons run within a retromalleolar groove on the back of the fibula and are held in place along the lateral malleolus by the superior peroneal retinaculum
- The tendons course superficial to the calcaneofibular ligament and then . . .
- Next to the calcaneus they may be separated by the calcaneus' peroneal tubercle, with the brevis anterior to the tubercle; or both may pass anterior to the tubercle
- The longus tendon crosses on the plantar aspect of the brevis before insertion
FUNCTION
- The Peronei are the major foot everters, using the lateral malleolus as a pulley
APPEARANCE ON MRI
- The brevis tendon is usually anterior, or less commonly medial, to the longus
- The brevis' musculotendinous jxn is more distal than the longus', so that just above the lateral malleolus the longus tendon can be seen lateral to the brevis muscle or tendon depending on where the musculotendinous jxn is
- At or above the retromalleolar groove, the longus tendon is usually rounded while the brevis tendon is usually more flat, though often at the groove the tendons often cannot be appreciated as separate structures (Fig 2)

Fig. 2 Normal Peroneal Tendons at the Retromalleolar Groove -- Axial T1-weighted image --The tendons often cannot be appreciated as separate structures. The thin black line posterior to the tendons is the superior peroneal retinaculum.
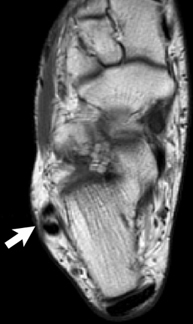
Fig. 3 Normal Peroneal Tendons Next to Calcaneus Superficial to Calcaneofibular Ligament -- Axial T1-weighted image -- Brevis is Anterior and Longus Posterior
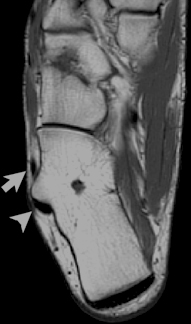 
Fig. 4 Normal Peroneal Tendons split at Peroneal Tubercle of Calcaneus -- Axial and Sagittal T1-weighted images -- Brevis is Anterior to the Tubercle (arrow) and Longus is Posterior (arrowhead)
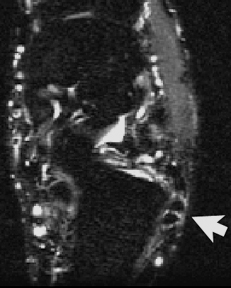 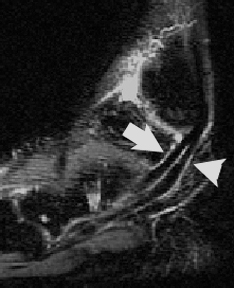
Fig. 5 Normal Peroneus Brevis (anterior, arrow) and Longus (posterior, arrowhead) Tendons -- Axial and Sagittal STIR Images -- Tendons are low signal with a normal small amount of fluid within the tendon sheath around them
PERONEAL TENDON DISPLACEMENT
-
The peroneal tendons can be displaced --subluxed or dislocated -- when the superior retinaculum is disrupted. This can occur with complex ankle fractures, calcaneal fractures, or with a forced inversion injuy with plantar flexion.
-
The diagnosis is made when tendons are lateral to the distal fibula rather than posterior to it (Fig 6).
-
Calcaneal and ankle fractures can also cause tendons to be torn or trapped between fracture fragments.
A B C
D E
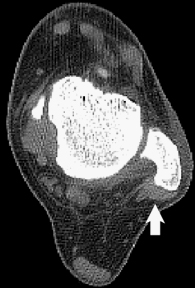
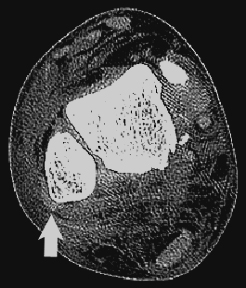
Fig. 6 Normal Location of Peroneal Tendons and Displaced Tendons on CT -- Normal tendon location is posterior to the fibula in the retromalleolar groove, as seen on axial (A) and consecutive coronal (B) CT images. When the tendons are displaced from a torn retinaculum they will move lateral to the fibula as seen on axial (D) and coronal (E) images in a patient with a calcaneal and hindfoot fractures.
PERONEAL TENDON TEARS
-
Tendon tears most often occur in the brevis. The longus tendon is partially torn in ~30% of brevis tears and infrequently torn in isolation.
-
In partial tears of the brevis tendon, there may be any combination of the following findings:
-
the tendon may become enlarged,
-
may lose its homogenous low signal, or
-
may have focal areas of increased T2/STIR signal.
-
Longitudinal tears of the brevis tendon are called peroneus brevis splits.
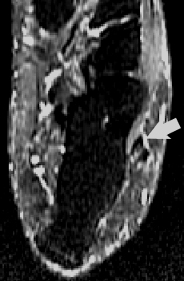 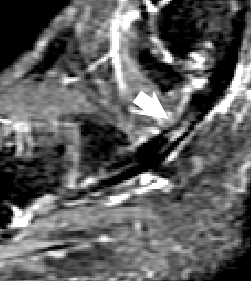
Fig. 7 Peroneus Brevis Split -- Increased signal is seen within the tendon on axial and sagittal STIR images over 1.5 cm portion just distal to the lateral malleolus.
-
Splits occur in patients of all ages and athletes. It may be dificult to diagnose clinically b/c of overlap with other ankle injuries and may be minimally symptomatic though pain and swellling are common.
-
Splits occur usually when in dorsiflexion as the brevis tendon is wedged between the lateral malleolus and taught longus tendon.
-
Thus most brevis tears begin at the lateral malleolus since that it is the main point of contact. Second most common location would be at the peroneal tubercle.
-
Usually brevis splits occur after chronic "wear and tear" frays the tendon from repetitive dorsiflexve stress culminating in a tear.
-
Tears can propogate distal or proximal to their origin.
-
Certain conditions predispose to splits, such as a shallow retromalleolar groove, lax or torn peroneal retinaculum, low lying brevis muscle belly, and the presence of a peroneus quartus muscle.
 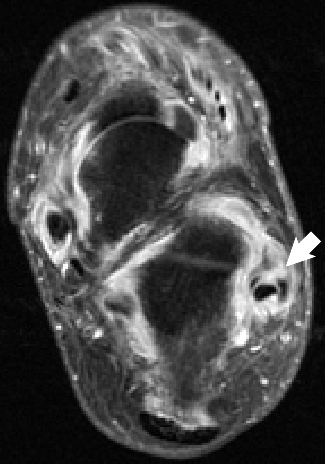
Fig 8 Peroneus Brevis Split -- Axial T1 image shows a C-shaped brevis tendon around the longus, a common appearance, just above the retromalleolar groove. More distal, on the axial STIR image, the tendon has split into 2 tendons. This was a patient with rheumatoid arthritis with marked tenosynovitis and an inflamed ankle joint as evidenced by the increased fluid in all compartments.
MRI Findings in Peroneus Brevis Splits
-
Splits can be seen as increased T2/STIR signal longitudinally along a part of the tendon
-
Also, more severely, the brevis tendon, which can normally be flat, will be C-shaped, V-shaped, or there will be 2 separate tendons and only 1 muscle body from a longitudinal tear.
-
Brevis splits are most commonly seen on axial images but sometimes you can be lucky and get the longitudinal tear on sagittal or coronal images
-
Again, one must be careful of "magic angle" phenoimenon as the tendons course below the fibula. Oblique axial images angled perpendicular to the peroneal tendons distal to the fibula can be very helpful in this regard.
 
Fig 9 Peroneus Brevis Split -- Axial Gradient image shows an enlarged brevis tendon with the appearnce of multiple small tendons from marked fraying and tears as the tendon passes the retromalleolar groove. Distal to the fibula the axial T1 image shows a split brevis with small round tendon posteriorly and C-shaped tendon anteriorly and inflamed tissue/fluid between.
-
You may see a fibular spur on the posterior lateral malleolus from reactive periostitis
-
One must be sure to distinguish a full split (2 tendons) from a bifurcated peroneus brevis tendon (there is a muscle belly for each tendon) and an extra tendon from the separate accesory peroneus quartus muscle.
Peroneus longus tears usually occur with brevis tears and have a similar appearance on MRI (Fig 10).
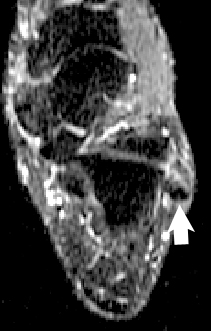 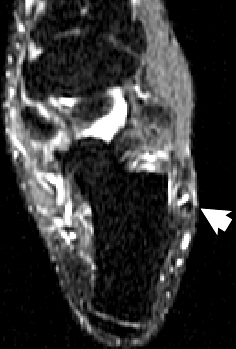
Fig 10 Peroneus Longus Split -- Axial STIR images show a cleft of increased STIR signal in the posterior aspect of the longus consistent with a small longitudinal tear. The brevis, medial on the left image and anterior on the right, also has high signal within it from a small tear.
References
Kaplan PA, Dussault R, Helms CA, Anderson MW, Major NM. Musculoskeletal MRI. Philadelphia, WB Saunders, 2001.
Discuss
|