| Home
About
|
Popliteus Muscle Injury
Print-friendly version of this page
Posted by mpsmith@u.washington.edu, 8/7/03 at 12:38:19 PM.
Popliteus Muscle

ANATOMY AND FUNCTION
- Its origin is on the
anterior portion of the popliteal groove on the lateral surface of the
lateral femoral condyle (anterior & inferior to LCL origin)
and another less strong origin is from the fibular head,
called the popliteofibular ligament. An
additional origin from the lateral meniscus can be seen in a
small percent of patients.
- The popliteus tendon courses under the lateral collateral ligament, descends into the popliteus hiatus, then passes under the arcuate ligament and becomes extraarticular before finally joining its muscle belly
- Its insertion is fan like on the posterior surface of the tibia above the popliteal line
- Its primary function is internal rotation of the tibia on the femur in the non weight-bearing state &, when weight-bearing, external rotation of the femur
on the leg. It helps with posterior stability of the knee in preventing
posterior translation of the tibia on the femur & prevents
excessive external and varus rotation of the tibia during knee
flexion. It is the main lateral stablizer of the knee.
POSTEROLATERAL CORNER
- The posterolateral region of the knee is often seen as a functional tendoligamentous unit, which is termed the arcuate ligament complex.
- This complex encompasses the popliteus muscle and tendon along with the lateral collateral ligament; biceps femoris tendon; popliteal meniscal and popliteal fibular ligaments; oblique popliteal, arcuate, and fabellofibular ligaments; and lateral gastrocnemius muscle.
- Injuries of the popliteus are infrequent and rarely isolated (less than 10%).
They usually occur as part of a posterolateral corner complex
injury, which is also frequently associated with injury of
the anterior or posterior cruciate ligament.
- It is important not to overlook popliteus and posterolateral injury in the presence of an anterior or posterior cruciate ligament injury, because the reconstructed cruciate ligament will likely fail without repair of the posterolateral injuries.
- Unrepaired popliteus injuries can cause severe disability from both instability and articular cartilage degeneration.
MECHANISM OF INJURY
- Athletic trauma, motor-vehicle accidents,and falls are the most common causes of injury of the posterolateralcorner of the knee.
- Rare isolated posterolateral injury can result
when a force is directed in a posterolateral direction against the
proximal anteromedial aspect of the tibia with the knee at or near full
extension, which produces knee hyperextension and varus bending that disrupts the posterolateral structures.
- Combined hyperextension and tibial external rotation forces can also produce posterolateral injury.
- Usually these forces are so severe orcombined with other forces to injure other ligaments in the knee.
- The varus
and hyperextension instability that results is frequently overlooked at
clinical examination or masked by more extensive injury symptomatology.
RADIOGRAPHIC EVALUATION
-
Radiographs with posterolateral injury may show abnormal widening of the lateral joint space, an arcuate fracture of the fibular head, avulsion of the Gerdy tubercle off the tibia, or a Segond fracture (avulsion of the lateral aspect of the capsule from the tibial plateau).
-
Although a Segond fracture is usually considered indicative of a tear of the anterior cruciate ligament, it also occurs in association with isolated posterolateral injury.
MR EVALUATION
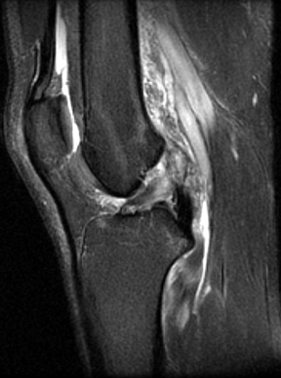
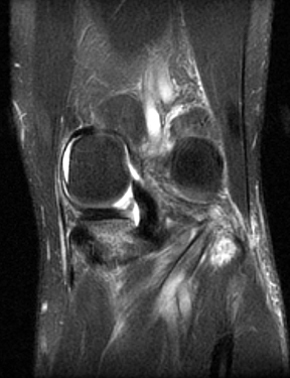
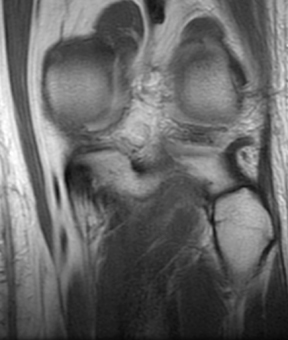
At MR imaging, popliteus lesions have different appearances depending on the level and grade of damage. They may appear as an avulsion of the popliteus tendon from its femoral attachment, as an irregular contour of the tendon at the popliteal hiatus with surrounding high-signal-intensity edema, or as swelling and high-signal-intensity changes within the popliteus muscle. A complete popliteus tendon tear may be seen as an interruption and possibly as retraction of the muscle belly, which may appear as a "mass" surrounded by fluid. Only fat should be present behind the popliteus tendon. Therefore, the presence of fluid posterior to the tendon should suggest a capsular tear if the existence of a fluid-filled popliteal bursa is taken into account.
The majority of popliteus tears are extraarticular, involving the muscular or myotendinous portion, although they can be intraarticular at the level of the popliteal hiatus and at or near the femoral insertion. Such injuries can also be a mixture of intraarticular and extraarticular
The popliteal bursa is an extraarticular extension of the synovial membrane of the knee joint extending from the popliteal hiatus along the proximal part of the popliteus tendon. On T2-weighted images, a fluid-filled popliteal bursa appears as a well-defined area of high signal intensity surrounding the popliteus muscle and tendon. This bursa may be confused with a tear of the popliteus muscle and tendon or of the posterior capsule.
In 95.8%
(23/24) of patients, the tears of the popliteus involved the muscular
portion. Three patients had tears of both the muscular and
tendinous portions or the tendon alone. The anterior and posterior
cruciate ligaments were torn in 16.7% (4/24) and 29.2% (7/24) of
patients, respectively. There were medial and lateral meniscal tears in
45.8% (11/24) and 25% (6/24) of patients, respectively. There were
injuries of the medial and lateral collateral ligaments in 8.3% (2/24)
and 4.2% (1/24) of patients, respectively. Bone bruises and/or
fractures were seen in 33.3% (8/24) patients. In 8.3% (2/24) of
patients, the popliteus injury was an isolated finding.
Avulsion injuries at the femoral insertion of the popliteus tendon have been reported. However, injuries of the muscle belly and myotendinous junction of the popliteus are far more common. Enlargement of the muscle and increased signal intensity on T2-weighted images can be demonstrated at MR imaging. MR imaging is also useful for differentiation of partial interstitial tear from complete muscle rupture, since the latter produces retraction and clumping.
Discuss
|