| Home
About
|
Psoriatic Arthritis
Print-friendly version of this page
Posted by klinnau@u.washington.edu, 10/16/03 at 9:16:58 AM.
Psoriatic arthritis (PsA)
- 2-17% of patients with psoriasis get arthritis
- skin lesions and arthritis are often asynchronous: 80-85% of pts have skin lesions first
- synovial inflammation leading to bony proliferation at joint margins
- inflammation at the ligamentous attachments: enthesopathy
Age of onset usually 30-45 years, no gender preference
Prognostic factors:
poor prognosis:
- late age of onset
- five or more effused joints
- high immunosuppressive medication use
good prognosis:
other labs:
- HLA B27 positive in 60-80% of psoriatic spondylitis and 20% of peripheral PsA
- CRP - usually elevated
- may be elevated: acute serum amyloid A (A-SAA)
- ANA may be mildly elevated
- Rheumatoid factor negative (or mildly elevated with titer<1/40, which is cut-off for Rheumatoid Arthritis (RA))
Hypothesis:
Joint damage occurs maximally during first 2 years of disease:
early diagnosis
aggressive treatment
Patterns of presentation:
- asymmetric oligoarthritis: > 50%
- polyarthiritis with predominantly DIP involvement (classic): 5-19%
- symmetric seronegative polyarthritis simulating RA: up to 25%
- sacroiliitis and spondylitis resembling Ankylosing Spondylitis (AS): 20-40%
- arthiritis mutilans with resorption of the phalanges: 5%
Onset may be
insidious (66%) or
acute (33%) mimicking gout or septic arthritis
Radiology findings:
Early findings:
- normal
- soft tissue swelling: sausage fingers or fusiform swelling about finger joint
- usually no osteoporosis (˙≠ RA)
- prominent erosions in marginal areas of joints
- Perisostitis in metaphysis and diaphysis
- asymmetric paravertebral ossification of thoraco- lumbar junction (from vertebral body to body ˙≠ AS: corner to corner)
- bone scans may show hot spots prior to radiographic abnormality
Distribution of radiographic findings:
- synovial or cartilaginous joints and tendon attachment of axial and appendicular skeleton (= Reiter = AS ˙≠ RA)
- unilateral or asymmetric (˙≠ RA) at the hands and feet
- upper and lower extremity joints (˙≠ Reiter: more commonly lower extremity only)
- DIP, PIP of hand and foot commonly affected
- Abnormal phalangeal tufts and calcaneus (characteristic)
- If axial skeleton: most commonly sacroiliac (SI) and spinal joints
General findings:
- Soft tissue swelling
- No osteopenia (˙≠ RA)
- Joint space may be widened or narrowed
- Severe marginal erosions gnawing away bone towards the center of the joint are typical
- Pencil-and-cup appearance of small joints of hand and feet (DDX: RA, leprosy, sarcoid)
- Bone proliferation (=other seronegative spondylarthropathies = gout): spiculated, frayed, paintbrush appearance (˙≠ RA: no bone deposition)
- Perisostitis in metaphysis and diaphysis (= Reiter= Juvenile RA =infection) sometimes accompanied by condensation of bone
- Intraarticular osseous fusion ( AKA bone anklylosis) (DDX: erosive OA, RA (carpus and tarsus), infection, other seronegative spondylarthropathies)
- Enthesopathy of calcaneus (Achilles tendon), femoral trochanters, ischial tuberosities, malleoli, olecranon, patella, femoral condyles.
- Tuft resorption of the distal phalanges of the hands and feet (characteristic) (DDX: scleroderma, thermal injury)
Erosions:
- Start at joint margins, tend to be severe
- Proceed centrally into joint
- Result in irregular osseous surfaces: lack of apposition of adjacent bone margins (˙≠ OA)
- Wrist abnormalities not so common in psoriasis
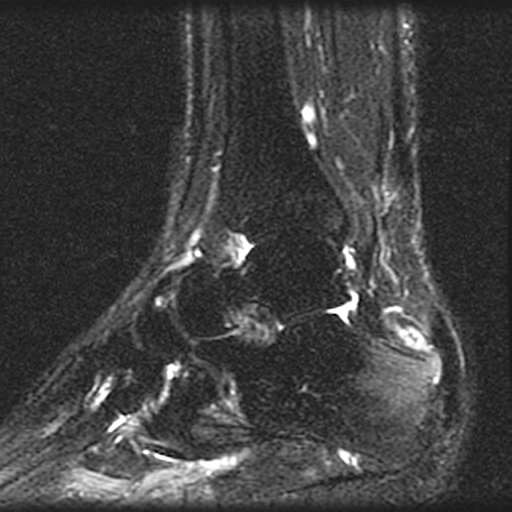
Calcaneus:
- Erosion and proliferation of posterior or inferior surface
- Radiodense area postero-inferior due to retrocalcaneal bursitis
- Achilles tendon may be thickened.
SI joints:
- 30-50% of patients with PsA
- erosions and sclerosis of SI joints
- bilateral lesions are more common than unilateral
Spine:
- asymmetric paravertebral ossification of lower thoraco- lumbar junction (from vertebral body to body ˙≠ AS: corner to corner)
- Syndesmophytes are greater in size, asymmetric distribution, away form vertebral column ˙≠ AS
- squaring of vertebral bodies, apophyseal sclerosis uncommon ˙≠ AS
- Cspine abnormalities may be extensive: facets, discovertebral,
proliferations along anterior surface, atlantoaxial subluxation, dens
erosions.
Scintigraphy:
- bone scans may show abnormality prior to radiographs
- asymmetric ˙≠ RA
- DIP, PIP >> SI, calcaneus
Discuss
|