| UW MSK Resident Projects |
|
|
|
|
Pigmented Villonodular SynovitisPrint-friendly version of this pagePosted by slogerfo@u.washington.edu, 5/3/04 at 8:46:29 AM.
PIGMENTED VILLONODULAR SYNOVITIS WHAT IS IT?
CLINICAL PRESENTATION:
IMAGING FINDINGS: Radiographs may be entirely normal or show minimal and non-specific findings. Classic radiographic appearances include bone erosions and single or multiple juxta-articular subchondral "cysts" and are commonly seen on both sides of the joint.
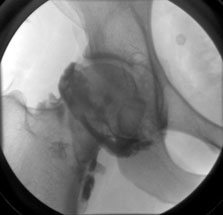
In the hip, bone lesions typically develop at the junction of the femoral head and neck, and acetabulum. Additionally, erosions are more commonly seen than in the knee due to the tight capsule of the hip joint.
In the bones of the hands and feet, where the localized nodular form prevails, the cysts appear as sharply marginated radiolucent defects in multiple bones.
Giant Cell Tumor of the tendon sheath in the wrist and toe is considered PVNS of the tendon sheath
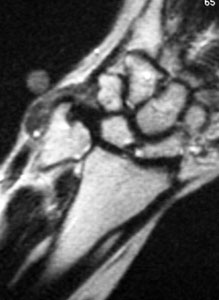
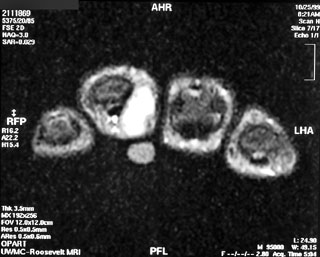
MRI is highly sensitive and specific for PVNS. Characteristic findings include joint effusion, low signal on both T1 and T2, and gradient echo secondary to hemosiderin deposition, hyperplastic synovium, bone erosions and preservation of bone density.
On CT, the cystic erosions appear as decreased signal of the marrow.
Arthrography is another imaging modality that can be used in the diagnosis of PVNS and may show a richly vascular process,increased articular cavity, joint effusion or synovial villae.
Bone scan with Tc Pertechnetate may be useful for detecting inflammation of the synovial membrane. DIFFERENTIAL DIAGNOSES:
TREATMENT:
REFERENCES:
|










|