| UW MSK Resident Projects |
|
|
|
|
Rheumatoid ArthritisPrint-friendly version of this pagePosted by frebeles@u.washington.edu, 8/26/04 at 10:49:19 AM.
GENERAL: Rheumatoid arthritis is the most common purely erosive inflammatory
arthropathy. Rheumatoid arthritis is generally symmetric and affects
proximal joints. There are no proliferative erosions as in erosive OA,
psoriatic or Reiter's arthritides. Rheumatoid arthritis rarely includes
any productive bone such as periostitis, enthesopathy, and osteophyte
formation unless there is secondary osteoarthritis present. Rheumatoid
factor is positive in 90-95% of the cases. Early in rheumatoid
arthritis the RF may be falsely negative, and in older patients, the RF
may be falsely positive. [MSK: The Requisites, 2nd edition, Manaster et
al] The characteristic radiographic features of rheumatoid arthritis
include soft-tissue swelling, periarticular osteoporosis, joint space
narrowing, articular erosions, and marginal erosions. The marginal
erosions are caused by the extension of pannus into synovial pockets
overlying regions devoid of articular cartilage (which would normally
protect against the toxic debris and inflammatory pannus in the
synovial fluid). [Musculoskeletal Imaging: Case Review, Josephy Yu,
2001] RADIOGRAPHIC FINDINGS: Within the Wrist: Early RA will demonstrate erosions in the distal radioulnar joint, ulnar styloid, radial styloid, and triquetro-pisiform joint (the latter are best seen on ball-catcher's view). Typically, the next erosions and joint space narrowing will occur in the carpal bones and MCP joints. Ligamentous rupture can lead to wrist instability resulting in ulnar translocation of entire carpus, scapholunate instability, and dorsal and volar flexion carpal instability (DISI and VISI).
Within the Elbow: Diffuse involvement of joint with extensive erosion in olecranon articulation and joint space narrowing with trochlea of humerus seeming to "dig into" olecranon. Joint effusion and olecranon bursitis may also occur.
Within the Shoulder: Glenohumeral joint space narrowing with marginal erosions within the humeral head. Ligamentous/tendinous injury results in rotator cuff degeneration with a "high-riding" humeral head. Also look for lysis of the lateral clavicle and erosion at the insertion of the coracoclavicular ligament.
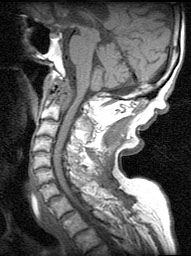
Within the Spine: The cervical spine is commonly affected; particularly look for C1-C2 involvement which can have catastrophic consequences. For instance, pannus formation near the odontoid can cause erosions in the odontoid and ligamentous laxity of the transverse ligaments. The latter results in increased predental space (greater than 2.5-3 mm which is upper limit of normal in adults) which can result in canal stenosis. Alternatively, the pannus itself can proliferate and directly compress the spinal cord. Also, ligamentous destruction can result in atlantoaxial impaction (ie. dens goes up into the foramen magnum along with Mr. Cord--Mr. Cord doesn't like that). Other findings include erosions within the facet joints.
And courtesy of Dr. Richardson: Within the Hip: Axial joint space narrowing leading to protrusio deformity at the severe end of the spectrum, diffuse osteoporosis, lack of osteophyte formation unless secondary OA occurs. In contradistinction, OA usually results in superolateral (ie. weight-bearing) acetabular joint space narrowing, normal bone density and osteophyte formation. Within the Knee: Joint space narrowing, osteoporosis, marginal erosions, without osteophyte formation unless there is secondary OA (do you see a recurring theme?). There may be a joint effusion with fluid tracking into the semimembranosus-gastrocnemius bursa (AKA Baker's or popliteal cyst). Occasionally there will also be patellar tendon rupture. Within the Feet: MTP joint erosions early on, particularly of the 5th MTP. Toe deformities that result include lateral deviation at the MCPs and hammer toes. Also look for retrocalcaneal bursitis with erosions in the posterior calcaneus; the retrocalcaneal fluid can obliterate the pre-Achilles fat pad (AKA Krager's fat pad).
REFERENCES:
|












|