| UW MSK Resident Projects |
|
|
|
|
Tarsal CoalitionPrint-friendly version of this pagePosted by preby@u.washington.edu, 11/25/03 at 8:52:56 AM.
TARSAL COALITION What is it? Tarsal coalition is an abnormal union between tarsal bones. The union can be osseous, fibrous, or cartilaginous. This causes abnormal articulation within the mid and hind foot which produces accelerated degenerative osteoarthritis of the hindfoot and midfoot. The frequency of tarsal coalition is approximately 1% and occurs in males more than females. It is bilateral in 25% of cases. These numbers are generally accepted and based on symptomatic groups. Recent post-mortem exams have been performed to attempt to discover the "true" incidence of tarsal coalition. Solomon, et al, report an incidence of non-osseous coalitions as high as 12.7%! How does it happen? Etiologies can be congenital or acquired. Congenital tarsal coalition is the most common and results from a failure of normal tarsal segmentation. Congenital tarsal coalition classically presents in the 2nd or 3rd decade of life as a painful flatfoot deformity also known as "peroneal spastic flatfoot." Acquired tarsal coalition can follow infection, trauma, surgery or inflammatory arthritis. Which bones are involved? The calcaneus, talus, navicular and cuboid are commonly affected. A frequent written boards question asks: Which is the most common tarsal coalition? The answer depends on who you ask. Resnick lists them in this order with the most frequent first:
MSK Requisites lists them this way:
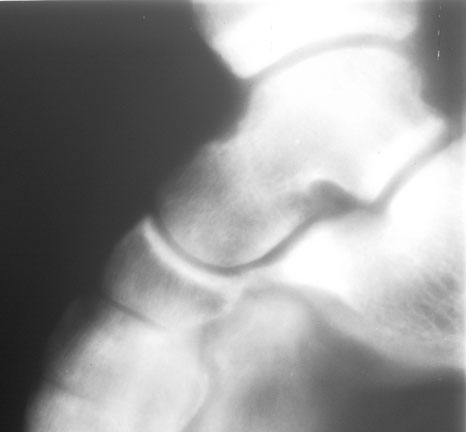
In general, calcaneo-navicular and talo-calcaneal are far more common than talo-navicular or calcaneo-cuboid. What are the imaging findings? Plain films classically demonstrate a number of bony abnormalities. These include: 1. The ant-eater sign: elongation of the anterior calcaneal process on the lateral view of the foot. This represents the bony bridging of calcaneo-navicular coalition.
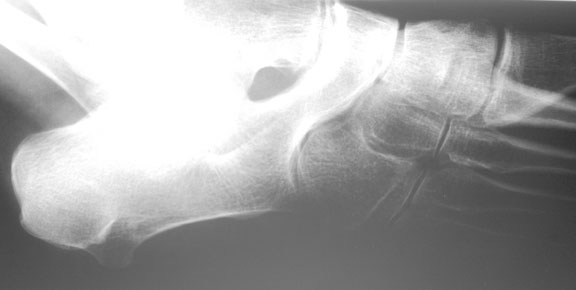
And you thought you would never see another plain film tomogram again (circa 5/3/72):
2. Talar beaking: dorsal beaking of the talar head may indicate underlying tarsal coalition, most commonly talo-calcaneal. However, it can also indicate Rheumatoid arthritis, DISH and acromegaly.
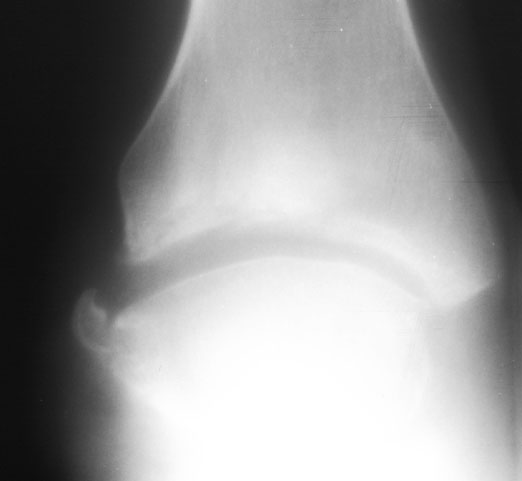
3. Ball-and-socket mortise joint: spherical remodeling of the talar dome. This occurs when the mortise joint gradually takes responsibility for abduction and adduction that is lost when the subtalar joint is fused in talo-calcaneal coalition.
4. Subchondral sclerosis, cortical irregularity and joint space narrowing: These are all indirect findings of fibrous or cartilaginous coalition.
Link to "Absent middle facet" AJR article on coalition, 2003. What are the imaging strategies? Calcaneo-navicular: A special 45 degree medial oblique projection will generally provide a clear view of the ant-eater sign in a complete osseous coalition. It will also show joint space narrowing, irregularity and sclerosis in a cartilaginous or fibrous coalition. Complete osseous: Cartilaginous or fibrous coalition: Talo-calcaneal: The Harris-Beath view, a penetrated posterior oblique image (aka, the penetrated axial view), with the patient standing on the cassette and the beam angled between 35 and 45 degrees to the cassette, is designed to reveal coalition between the sustentaculum and the talus at the middle facet.
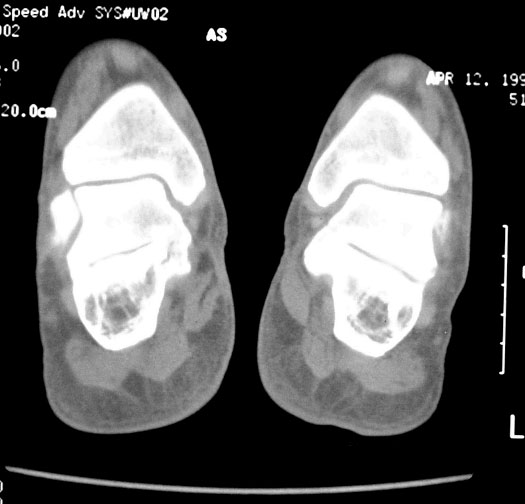
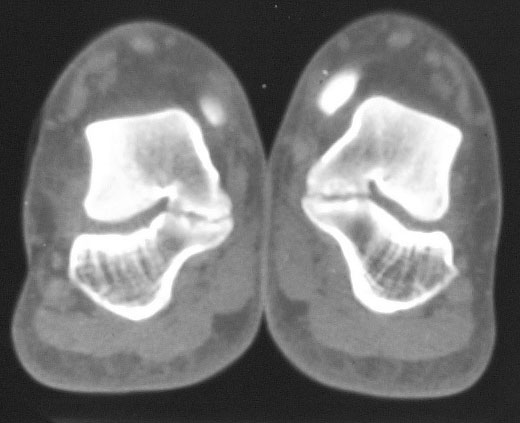
CT is usually definitive. It will clearly show any osseous coalition. It will also demonstrate the joint space narrowing, sclerosis and irregularity of cartilaginous or fibrous coalition.
Bone scan is sensitive but less specfic. It will show uptake in multiple elements of the hindfoot and midfoot because of altered mechanics and weight-bearing. [Picture here.] What difference does it make? What can we do about it? Most patients with tarsal coalition have a fixed hindfoot valgus of varying severity and some loss of the normal longitudnal arch. Peroneal muscle tightness develops and the patient complains of vague dorsolateral foot pain centered on the sinus tarsi, difficulty walking on uneven surfaces, foot fatigue and occasionally a painful limp. There are three common therapeutic options for calcaneo-navicular coalition.
And the therapies for talo-calcaneal coalition:
References: Campbell's operative orthopedics. Canale ST, Campbell WC, eds. 10th ed. Mosby, 2002. Musculoskeletal imaging: the requisites. Manaster BJ, et al. 2nd ed. Mosby, 2002. Diagnosis of bone and joint disorders. Resnick, D, 4th ed, WB Saunders, 2002. Liu PT et al; Absent middle facet sign: a sign on unenhanced radiography of subtalar joint coalition. AJR;181(6):1565-1572. Solomon LB et al; A dissection and computer tomograph study of tarsal coalitions in 100 cadaver feet. J Orthop Res. 2003 Mar;21(2):352-8.
Many images courtesy of Dr. Melvin Figley's University of Washington teaching file. |






|