Anatomy and Pathology
Interactive CT Anatomy Learning Module | University of Washington
| Home | Congenital | Inflammatory | Trauma | Tumor | Interactive Atlas | Quiz |
| Tumors and Tumor-like Conditions |
|
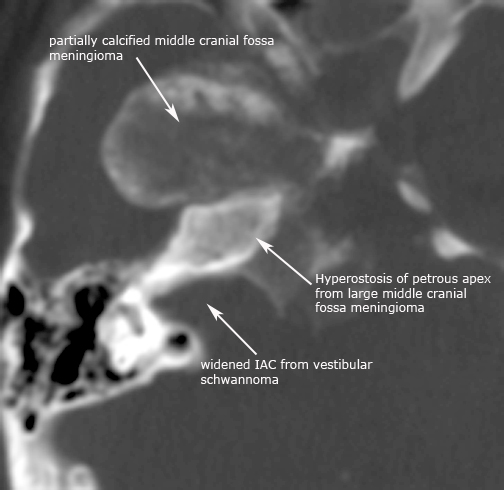
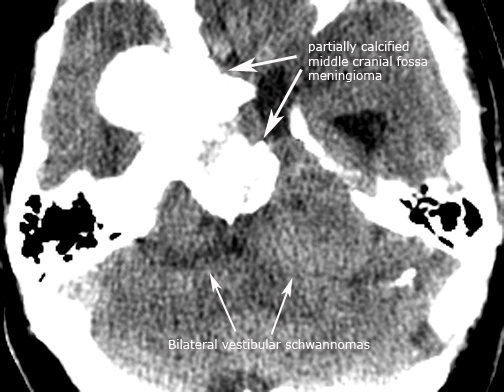
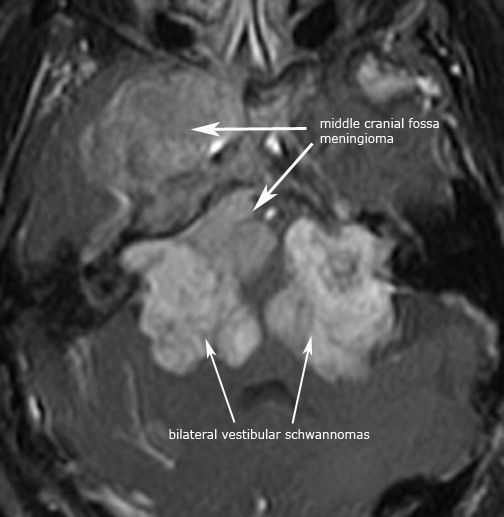
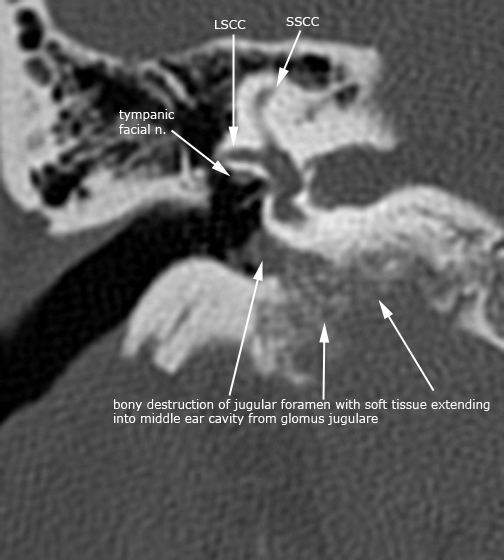
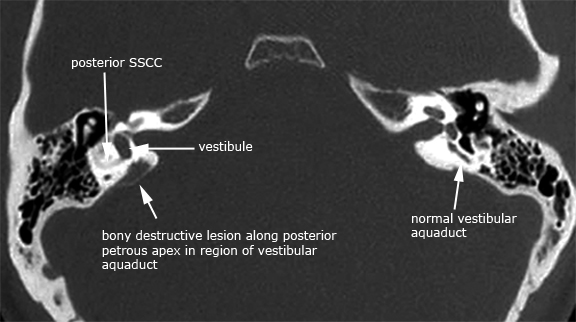
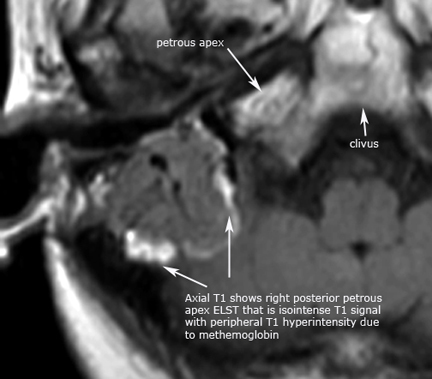
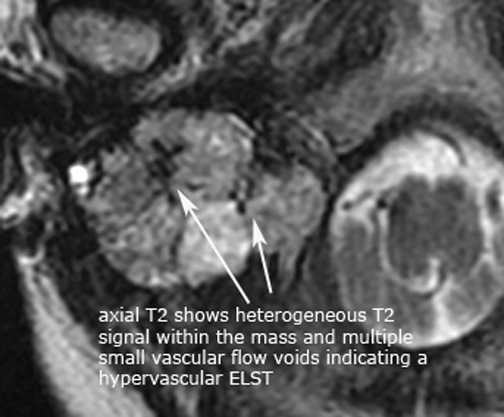
There are many types of tumors that affect the temporal bone, including intra-cranial tumors of the cerebellopontine angle that involve the 7th and 8th cranial nerves and internal auditory canal (IAC). Temporal bone imaging for tumors is typically evaluated based on the patient's presenting clinical symptom. The four most common clinical problems include 1) sensorineural hearing loss, tinnitus, or vertigo usually to evaulate for a vestibular schwannoma or other CPA angle mass; 2) pulsatile tinnitus or cranial neuropathy involving the jugular foramen; 3) peripheral facial nerve dysfuntion; 4) previously clinically identified tumor of the temporal bone. There are also non-neoplastic conditions, including various otodystrophies, that can mimic a neoplasm on imaging. The most common tumor to affect the temporal bone or related structures is the vestibular schwannoma, and less commonly the schwannoma can be isolated to the facial nerve as a facial schwannoma. A schwannoma is a benign, slow growing neoplasm arising from the nerve sheath and is composed of Schwann cells in a collagenous matrix. Vestibular schwannomas can occur in isolation, and is associated most commonly with Neurofibromatosis (NF-2). A less common tumor to occur in the CPA and may involve the temporal bone is the meningioma. This tumor is also seen in association with NF-2, but can occur in isolation elsewhere in the cranium including more commonly the olfactory groove, sphenoid wing, planum sphenoidale and supratentorially. Paragangliomas are the second most common tumor to involve the temporal bone and the most common tumor of the middle ear. These tumors originate from paraganglia along the tympanic branch of the glossopharyngeal nerve(Jacobsons' nerve) and the auricular branch of the vagus nerve (Arnolds' nerve), and within the intravagal paraganglia inferior to the foramen. The tumors are highly vascular and the glomus jugular can result in bony destruction as the tumor grows. Endolymphatic sac tumors (ELST) occur along the posterior petrous apex involving the vestibular aquaduct. These tumors are locally invasive papillary cystadenomatous tumors arising from the endolymphatic sac. ELST can occur sporadically, but are more common in patients with von Hippel-Lindau disease (VHL). The tumors cause local bony destruction as they grow and are hypervascular tumors with intra-tumoral hemorrhage commonly seen on MR imaging. Otospongiosis (aka otosclerosis) is an unusual disease affecting the otic capsule resulting in progressive hearing loss. The disease is typically characterized by autosomal dominance inheritance with variable penetrance and expression, and affects women more than men. In otosclerosis the normal endochondral bone of the otic capsule is replaced by spongy vascular irregular bone. There are two categories of otospongiosis: fenestral and retrofenestral (cochlear). The more common fenestral type affects the lateral wall of the bony labryinth including the both the oval and round window, promontory and facial nerve canal. The less common retrofenestral type primarily involves the cochlea, but usually has fenestral involvement. Fibrous dysplasia is an inherited disorder affecting the bones and can be mono-ostotic or poly-ostotic. The disease is characterized by the inability to form mature lamellar bone due to disordered osteoblastic activity. As a result there is gradual replacement of normal bone by an abnormal proliferation of isomorphic fibrous tissue elements intermixed with irregular trabeculae of woven bone. This results is bony expansion which can cause bony narrowing of the vascular channels and neuroforamen, and structurally weakened bone. There are three types of fibrous dysplasia with variable apperance depending on the mixture of fibrous tissue and osseous elements: Pagetoid, sclerotic and cystic. The following few cases highlight some of the more common tumors and otodystrophies to affect the temporal bone: schwannomas, meningiomas, paragangliomas, endolymphatic sac tumor, otospongiosis (otosclerosis), and fibrous dysplasia. There are also two uncommon bony tumors to arise from the temporal bone and are an osteochondroma and aneurysmal bone cyst. Case 1. IAC schwannoma and meningioma in patient with NF-2 (axial CT in bone window, axial NECT in soft tissue window, and axial T1 gad MR)
Case 2. Right geniculate ganglion facial nerve schwannoma (axial CT in bone windows and Cor T1 gad MR)
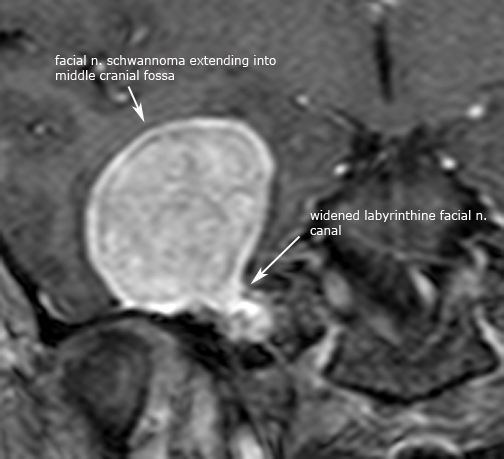
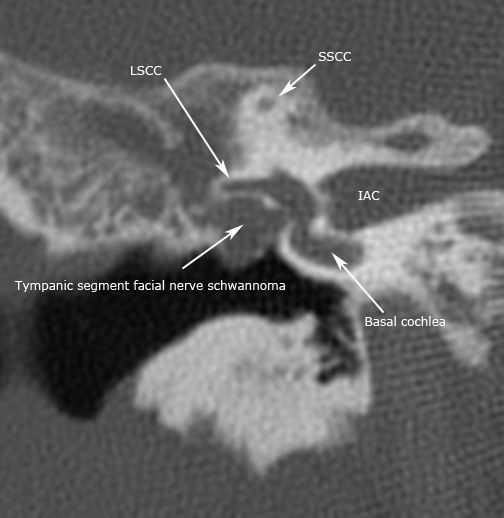
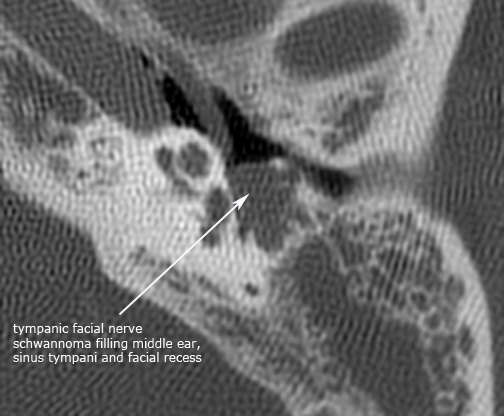
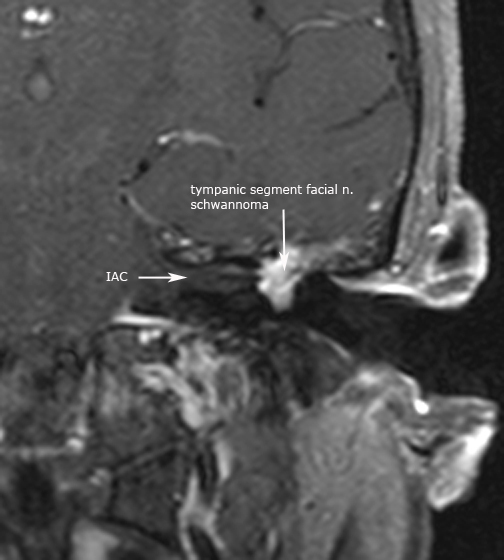
Case 3. Left tympanic segment facial nerve schwannoma (cor CT in bone window, axial CT in bone window, Cor T1 gad MR)
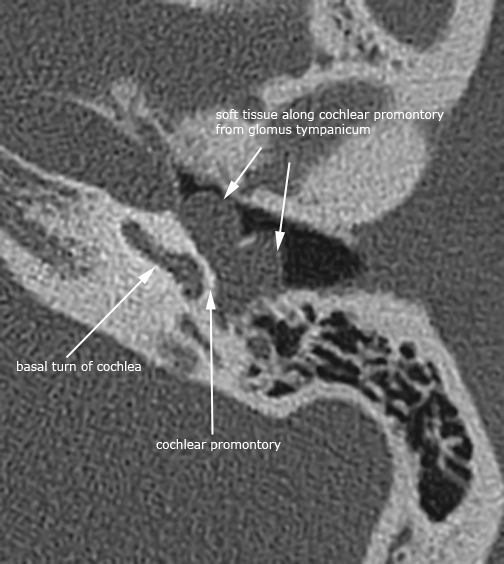
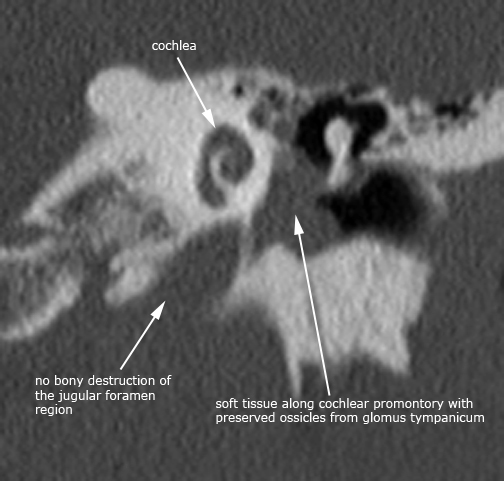
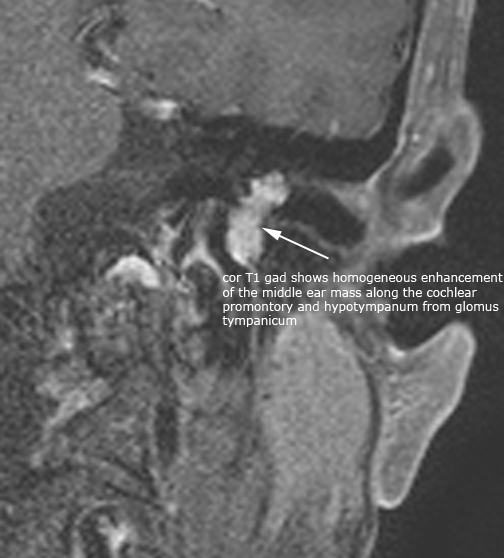
Case 4. Glomus tympanicum (axial and coronal CT in bone window, Cor T1 gad MR)
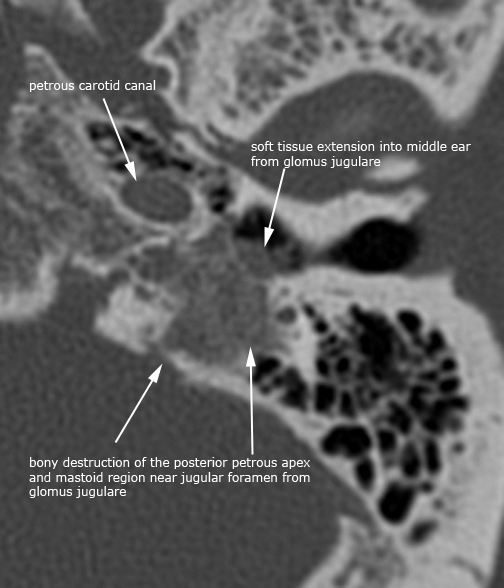
Case 5. Glomus jugulare
Axial and coronal T1 gad MR images
Case 6. Endolymphatic sac tumor (axial CT in bone windows, axial T1 and T2 MR images)
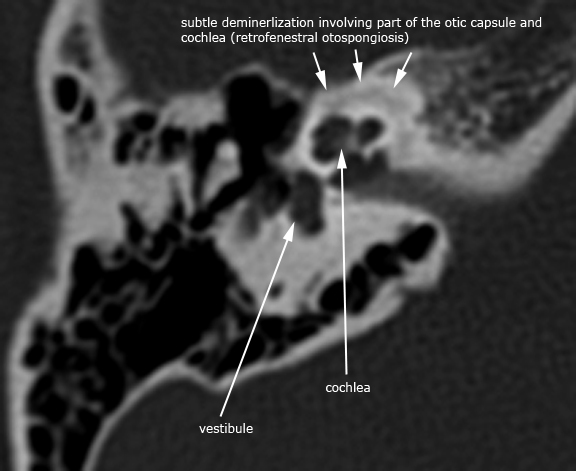
Case 7. Early otospongiosis (retro-fenestral)
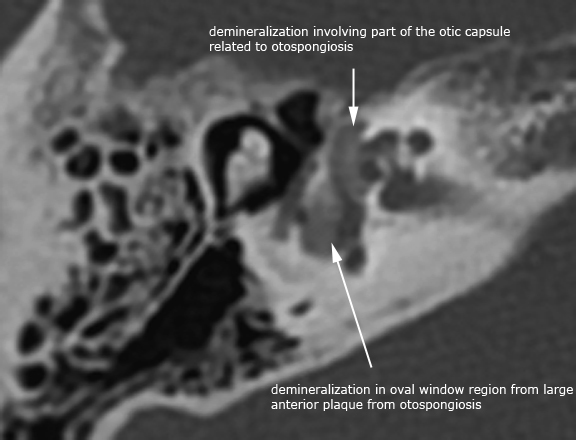
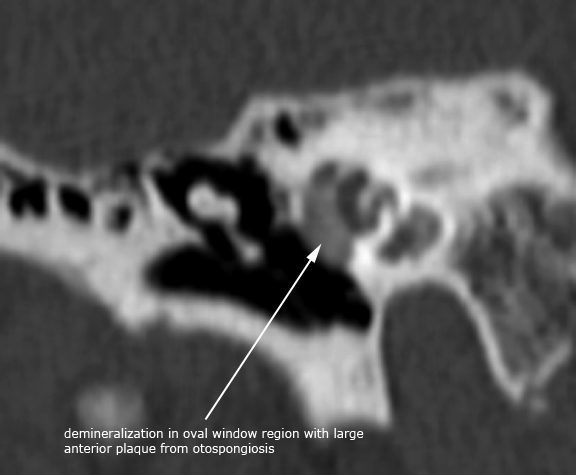
Case 8. Otospongiosis (fenestral and retro-fenestral)
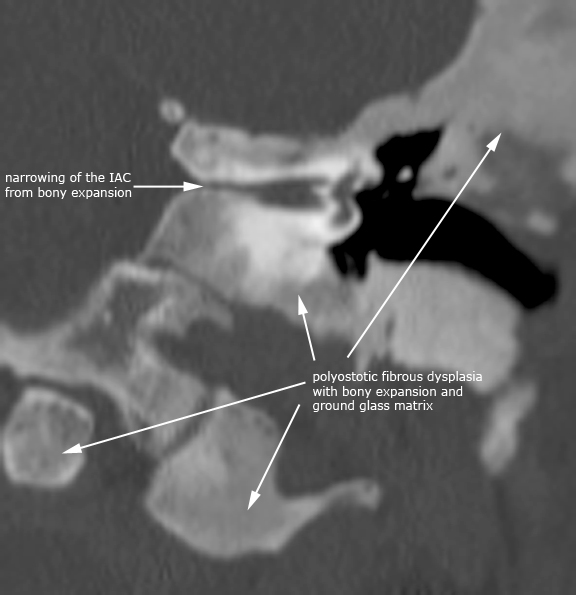
Case 9. Polyostotic fibrous dysplasia
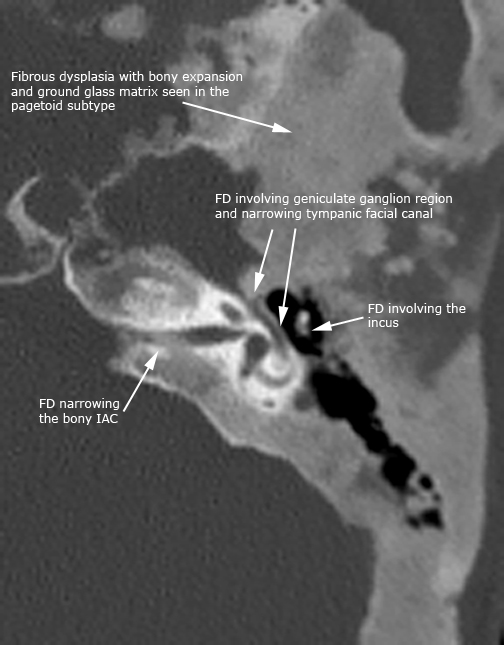
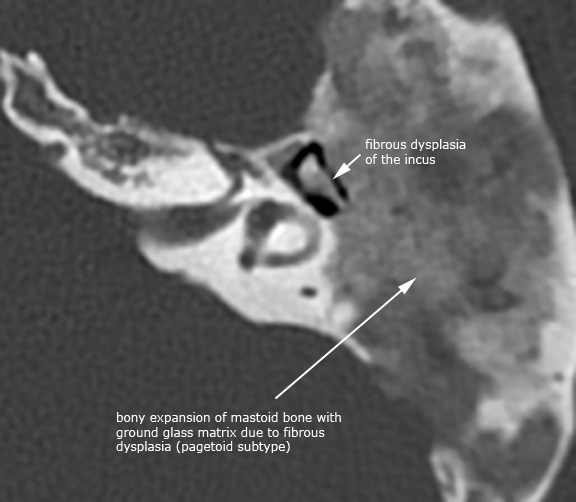
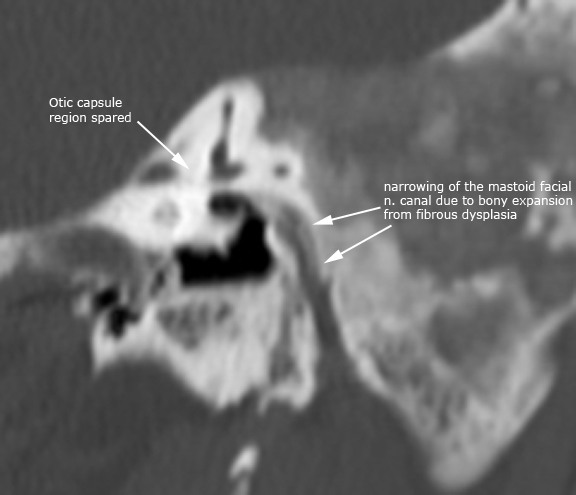
Case 10. Fibrous dysplasia affecting the ossicles and facial nerve canal
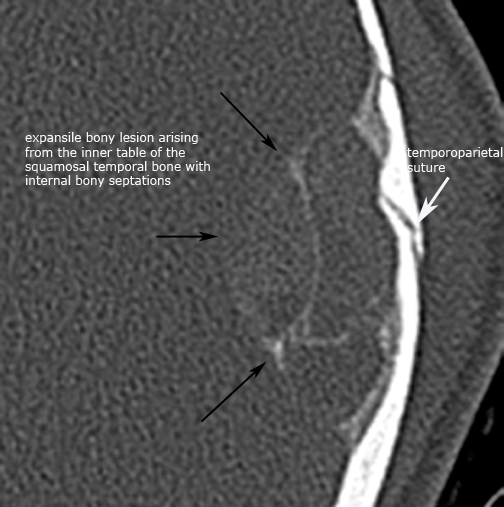
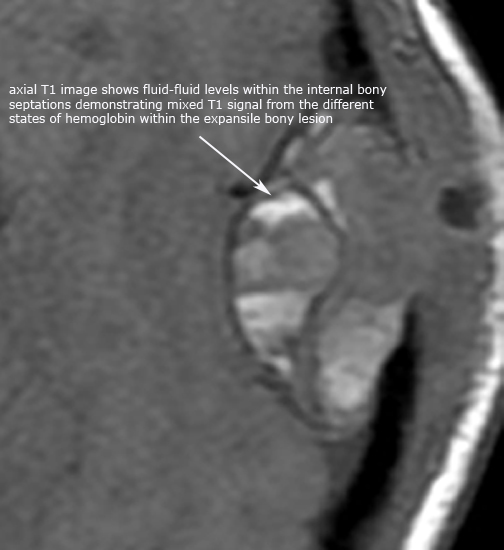
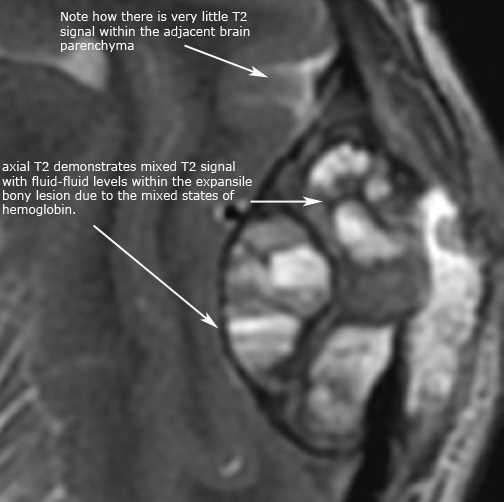
Case 11. Aneurysmal bone cyst of the temporal bone (axial CT in bone window, axial T1 and axial T2 MR images)
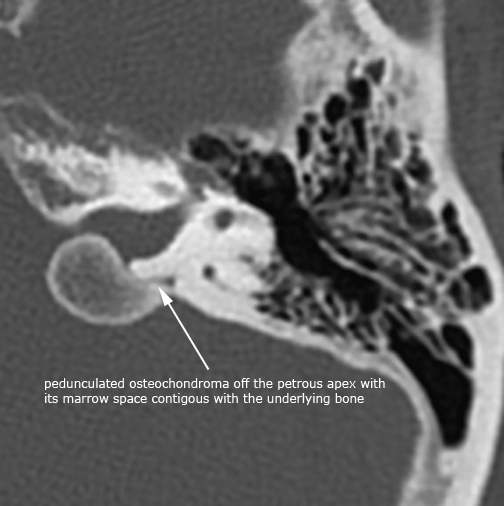
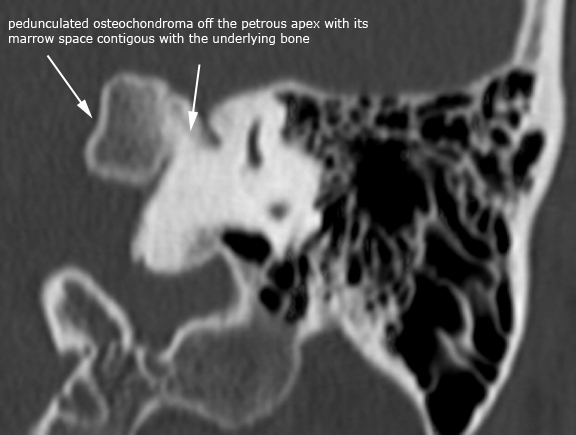
Case 12. Osteochondroma
|